The DHIS2 Annual Conference takes place from 15-18 June 2026! Learn more
The DHIS2 Annual Conference takes place from 15-18 June 2026! Learn more
The HEARTS in the Americas initiative aims to reduce premature mortality from noncommunicable diseases by 30%, and uses DHIS2 to help drive data use and informed decision making for cardiovascular disease prevention and treatment across the region.
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality in the Americas, and hypertension is the most significant modifiable risk factor. However, hypertension control rates remain low, and CVD mortality has become stagnant after decades of continuing reduction. The HEARTS in the Americas initiative, spearheaded by the World Health Organization, is a concerted response to the increasing prevalence of cardiovascular disease in the region. Managed by the Pan American Health Organization (PAHO) and funded by Resolve to Save Lives, HEARTS in the Americas aims to elevate the standard of cardiovascular health care across the continent, and in particular, to empower health centers to access their data and use it for decision making.
The HEARTS in the Americas team uses DHIS2 as a data warehouse for its monitoring and evaluation system and as a data entry tool, providing access for health care teams to report and evaluate their own data. The project aims to reduce premature mortality from noncommunicable diseases by 30% by 2030, a commitment made by all countries in the region in line with United Nations’ Sustainable Development Goal Target 3.4. According to a report from PAHO, “the System for Monitoring and Evaluation of HEARTS in the Americas is a tool for quality management based at the primary health care center. Developed under the open-source platform DHIS2, it allows health teams to report the variables linked to their professional practice and obtain periodic reports that enable them to evaluate their performance and results.”
As of the end of 2024, 33 countries in the Americas and the Caribbean have agreed to integrate the HEARTS in the Americas program in their primary healthcare networks, and El Salvador, Chile, Argentina, Cuba, the Dominican Republic, Ecuador and Grenada have already begun implementing DHIS2 for cardiovascular disease data. A related project in Guatemala, which uses the HEARTS approach but through independent implementation and a locally-owned DHIS2 instance, has helped achieve a four-fold increase in hypertension treatment rates, and a 14% increase in patients achieving blood pressure control.
“We want to break the paradigm that data for decision-making is only seen in the Ministry of Health” – Dan Angelo Gamarra Minaya, a PAHO consultant for the HEARTS project

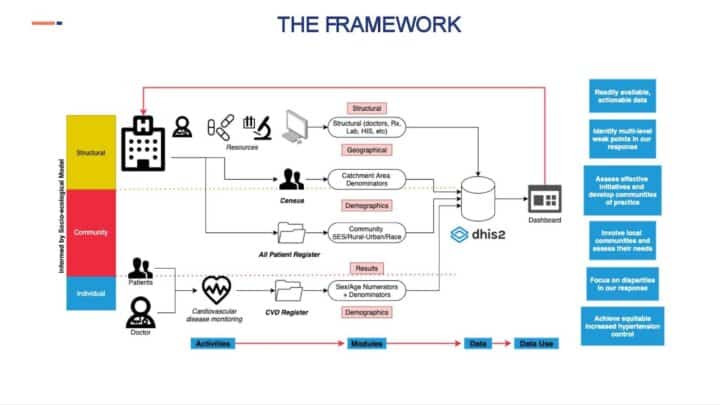
The project envisions a transformative approach in managing and preventing critical risk factors such as hypertension and diabetes, and encouraging countries to adopt the normative guidance from WHO as described in the Drivers and Scorecard HNT Control paper. This includes collecting and monitoring data points such as diagnosis, treatment, continuity of care, delivery system, and system for performance evaluation, on a personal and population level. “By capturing the right variables and ensuring that the country can produce the indicators described in the guidance, we can help accelerate interventions to curve hypertension and diabetes at facility level,” said Libardo Rodriguez, a PAHO consultant on the HEARTS project.
In general terms, the implementation of the HEARTS monitoring and evaluation system has begun in some countries and is progressing gradually in others. It has been essential to identify the gaps that hinder the regular use of the platform. One challenge that has been identified through experiences in implementing countries, is the gap between national health information systems and the variables and indicators proposed by HEARTS. Because many countries in the Americas use proprietary software for health management, it can be difficult to change existing processes and configurations. “Just to change a single variable can cost thousands of dollars as countries have invested in proprietary software that can only be modified by the company which created it, so we needed to find a solution which was flexible, scalable and open source,” Gamarra Minaya said.
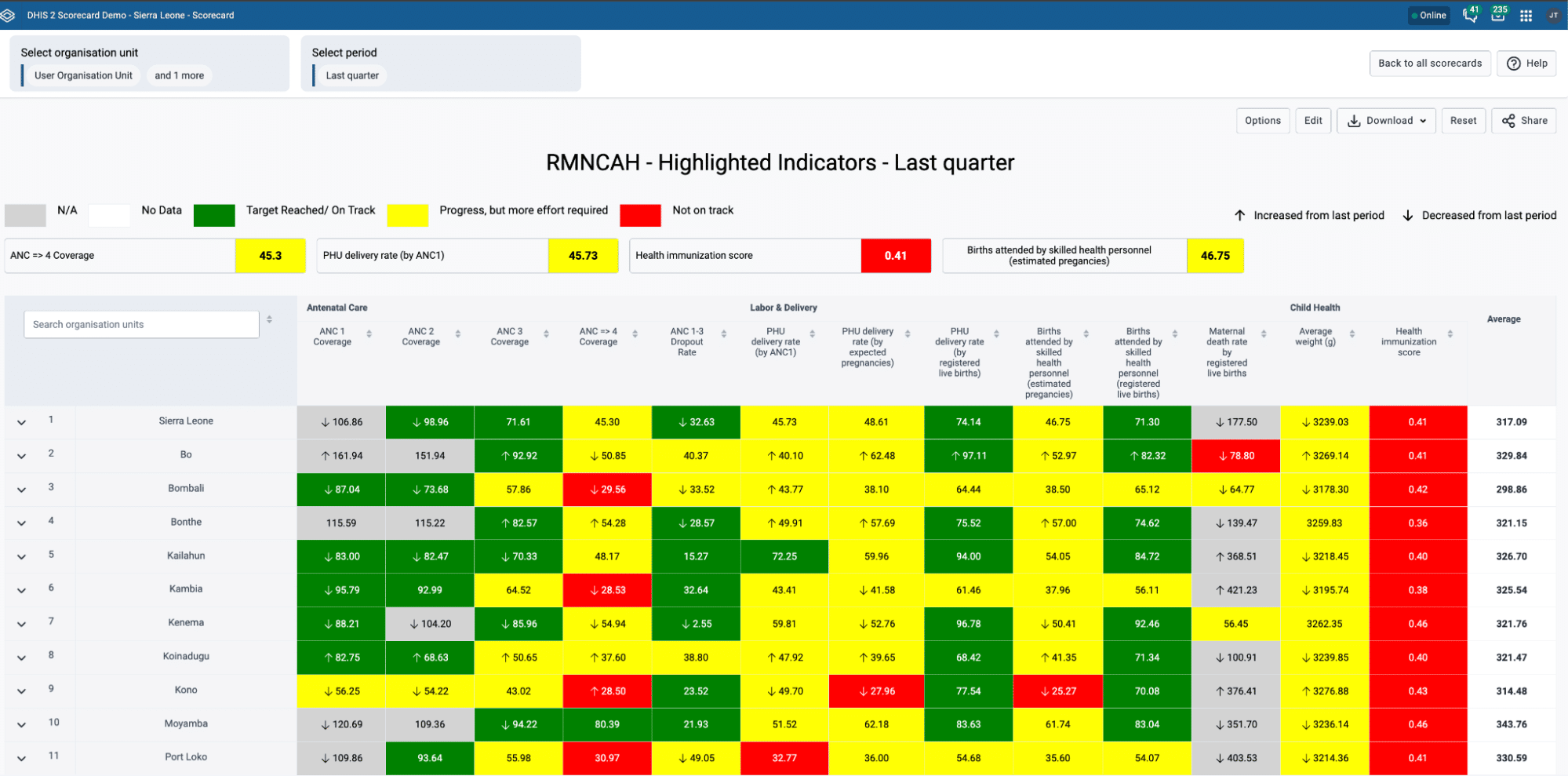
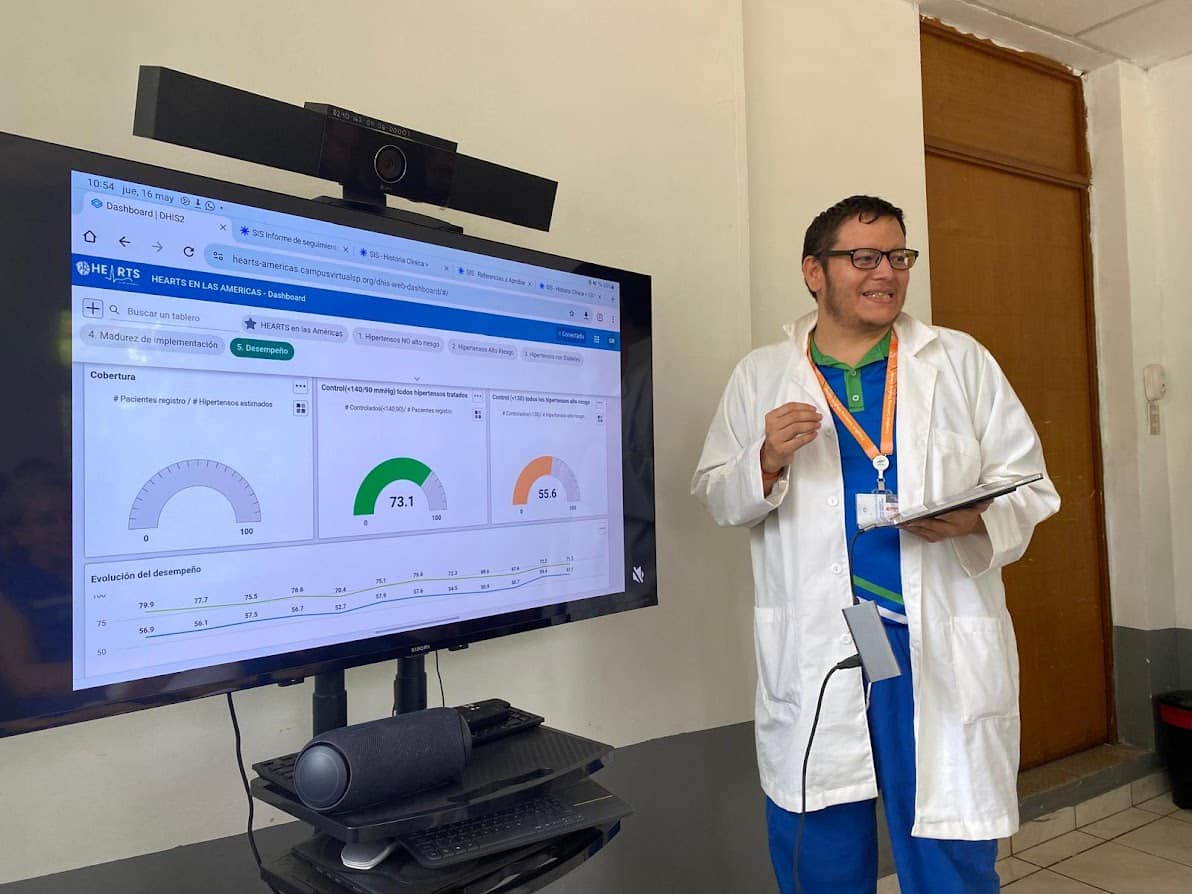
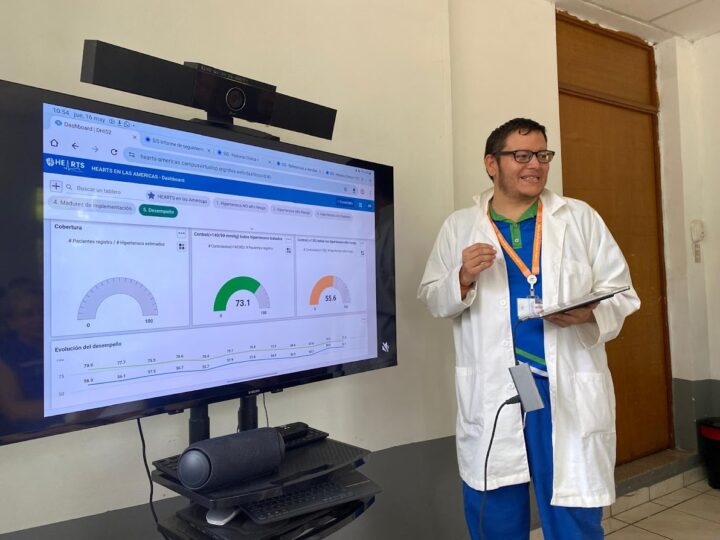
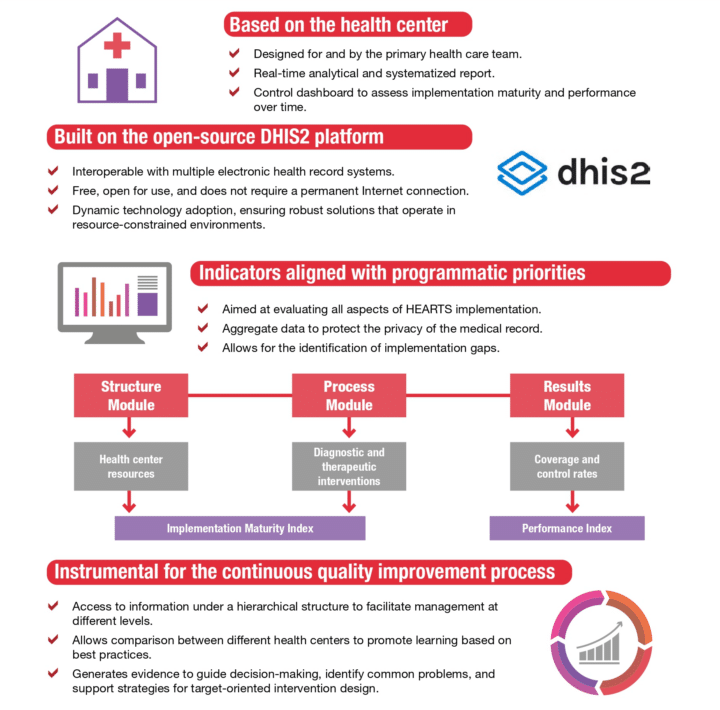
While some countries have managed to adapt existing systems to the recommended indicators, the HEARTS project offers countries a regional instance of DHIS2 as an alternative solution to gather and monitor their facility data. The team has created an aggregate dataset at facility level where monthly indicators can be then rendered in dashboards at facility, district and country level. “The platform has been designed as a user-friendly interface, especially for primary health care centers. This system, based on the DHIS2 platform, integrates all HEARTS quality indicators in its process module. It also automates report generation, allowing health centers to efficiently identify deficiencies and best practices in clinical management” PAHO said of its monitoring and evaluation system.
To date, 33 countries in Latin America and the Caribbean have agreed to integrate the HEARTS in the Americas program in their primary healthcare networks by 2025, and the approach has shown some positive outcomes, according to a journal article in Current Hypertension Reports. “The increase in hypertension coverage and control in primary health care settings compared with the traditional model is promising and confirms that the interventions under the HEARTS umbrella are feasible and acceptable to communities, patients, providers, decision-makers, and funders” the article’s authors said.
El Salvador has been a leader in adopting the HEARTS strategy, being the first country to use the DHIS2 platform to monitor the performance of its primary health care network, with 759 health centers now reporting with the system. It is now able to comprehensively assess the impact of the drivers on coverage and hypertension control rates in most of its primary care centers. In Chile, health officials began a gradual implementation of the system with the Semi-Annual Structure module for 29 health services. They conducted three training sessions for cardiovascular health care providers, focused on access and user creation to assign profiles to primary care centers.
In the province of Tierra del Fuego, Argentina, officials provided training for the regional supervisors from 11 primary health care centers. The process included collecting information from the semi-annual structure module, also covering some variables from the process and results modules. The close collaboration with the technology team is highlighted to ensure the inclusion of 100% of the indicators in the records, as well as work on interoperability to directly upload information into the HEARTS monitoring and evaluation system.
HEARTS has also recently made progress in Cuba, the Dominican Republic, Ecuador and Grenada. In Cuba, HEARTS is collecting data from 30 clinics, representing every province in the country, with a goal of onboarding 450 primary care centers in the first half of 2025. In the Dominican Republic, 703 of the country’s 1,774 primary care centers currently implement the HEARTS strategy, and officials plan to further enhance interoperability with clinics that access the national information system. Ecuador is now home to a pilot project for collecting cardiovascular disease data in DHIS2, with the goal of extending implementation across a broader geographic area and importing that aggregate data into the HEARTS platform. Grenada has taken a slightly different approach, using the HEARTS metadata to implement their own DHIS2 instance.
Additionally, a similar independent project in Guatemala, which collects individual data and uses a separate DHIS2 instance—not in the HEARTS M&E system—has yielded “a 4-fold increase in treatment rate and a 14% absolute increase in the proportion of patients achieving blood pressure control,” according to an article in the Journal of Hypertension. “The availability of free antihypertensive medications was enhanced through the (Ministry of Health) and the revolving-fund pharmacy, improving adherence in 37%. Additional process outcomes include: 28 health personnel received training on hypertension clinical management; 16 self-help groups for hypertensive patients were supported; 178 patient visits were tracked in the DHIS2 monitoring system.”
The HEARTS in the Americas initiative continues to operationalise global guidelines and build on existing implementations in the Americas. The project is seeking opportunities to expand to new countries, as well as disseminate the methodology towards other regions.
“The HEARTS M&E platform is in line with the principles of interoperability and scalability. The flexibility allowed by aggregate data collection improves scalability to multiple health systems as the program and data needs grow. DHIS2 modules can be extended and adjusted to meet new programmatic considerations or changes in indicators.” according to an article about the HEARTS M&E system published in the Pan American Journal of Public Health in 2022.