Turbocharging Malaria Surveillance with DHIS2 for electronic Integrated Disease Surveillance and Response in Tanzania
Tanzania leverages a DHIS2-based eIDSR to improve data accuracy in its national malaria control program to 93.9% and reduce presumptive malaria treatment by 30%
Tanzania, like most countries in Sub-Saharan Africa, is a malaria-endemic country. A majority of the population in mainland Tanzania live in high malaria transmission areas, accounting for 3% of global malaria cases and 4.1% of malaria-related deaths. The Ministry of Health (MoH), through the National Malaria Control Program (NMCP), has sustained a mix of strategies to curtail malaria transmission in the country including rapid diagnosis and case management, drug-based prevention, integrated malaria vector control and effective case-based surveillance. These efforts are enabled by government funding with the support of organizations like The Global Fund and PMI which provide more than 90% of donor funds in support of malaria control initiatives in Tanzania, and technical support from local partners including HISP Tanzania and the University of Dar es Salaam (UDSM) DHIS2 Lab.
Underlying these strategies is an effective Integrated Diseases Surveillance and Response System (IDSR) which has helped the MoH keep track of malaria transmission patterns and target interventions more efficiently. In 1998, Tanzania adopted the IDSR strategy based on the World Health Organization (WHO) guidelines, adapting them to the local context to monitor 13 priority diseases, including malaria. Several iterations of these guidelines have helped streamline and upgrade surveillance initiatives, making them more effective and impactful. DHIS2 is used for both the national HMIS and IDSR systems, which are integrated with each other and utilized by the MoH to collect, organize and visualize multi-level malaria surveillance data for intervention guidance.
The eIDSR system has helped MoH extend malaria surveillance to cover all of mainland Tanzania, including areas with limited internet connectivity. Data quality has continually improved, with data completeness at 93.9% in 2021, up from 90% the previous year. Health managers have also noticed increased positivity yield from malaria tests indicating that surveillance data is now more accurate, driving presumptive malaria treatment down by almost 30%.
Effective disease surveillance through distributed data collection strategies using DHIS2 and mobile phones
Tanzania has achieved significant success in malaria control over the years. These successes are most notable in the semi-independent islands of Zanzibar where malaria management is in the elimination phase with less than a 1% transmission rate as of 2020. However, the situation in mainland Tanzania differs remarkably, with a transmission rate of 14%, putting it still in the control phase of the malaria elimination continuum. In its bid to effectively control malaria in the country, a national goal to reduce malaria prevalence from 7.5% to 3.5% by 2025 was established. To achieve these targets, the MoH implemented an electronic IDSR (eIDSR) leveraging mobile telephony. The decision to implement the eIDSR was aimed at circumventing the challenges associated with manual IDSR methods, including slow reporting timelines, poor data quality, and limited tools for data sharing and analysis.
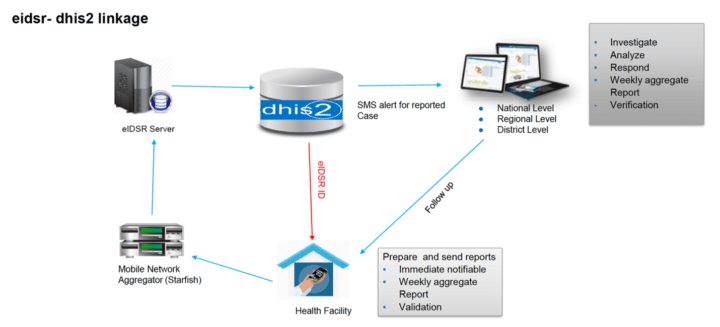
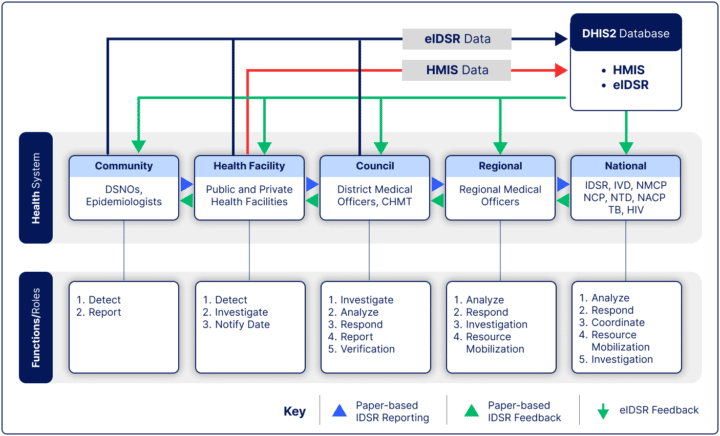
The eIDSR was developed in collaboration with the UDSM DHIS2 Lab and used an Unstructured Supplementary Service Data (USSD) application to transmit data to the DHIS2 platform for subsequent analysis and reporting. Given that Tanzania has a mobile phone usage rate of 86 per 100 people, and cell phone service coverage for most of the country, the initiative to use USSD has facilitated easy data collection from remote parts of the country where internet connectivity may be lacking or unreliable. Malaria data from health facilities are collected using mobile devices in USSD formats and sent to a mobile network aggregator which manages the data transmission to the eIDSR server. The eIDSR server aggregates and organizes the data before sharing it with the DHIS2-based HMIS for multi-level analysis and visualization. Once in the HMIS, the server notifies principal health officials of reported priority disease cases via SMS. They then follow up with the healthcare facility for information sharing, intervention planning and data use.
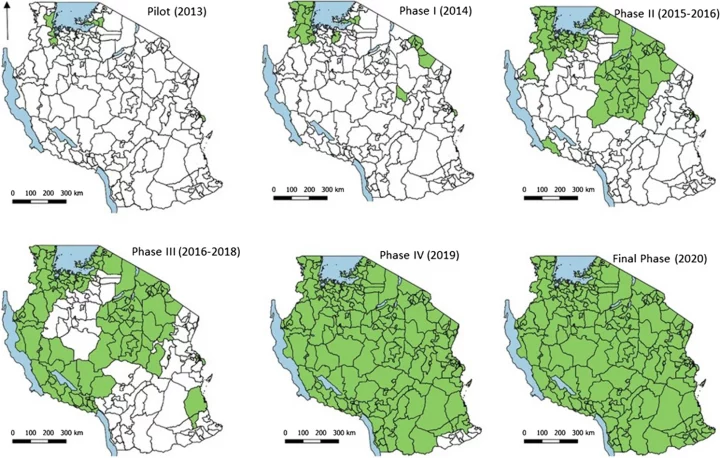
In 2013, the eIDSR platform was piloted in mixed urban and semi-urban settlements of Temeke Municipal Council in Dar es Salaam, covering 67 public and private health facilities. After a successful month-long implementation in Temeke, the pilot was extended to health facilities in Lake Zone districts for additional 3 months, bringing the total number of health facilities for the pilot to 182. This pilot afforded developers and administrators the opportunity to explore the system’s capabilities and make necessary adjustments before a national rollout. Following the successful pilots, the MoH commenced a phased rollout of the eIDSR throughout mainland Tanzania starting with Kagera region, which had the highest malaria burden in the country. The full roll-out took place over the following seven years, and was completed in January 2020, achieving 100% nationwide coverage in 7,471 public and private health facilities.
Beginning in 2021, a custom Android application developed by the UDSM DHIS2 Lab is being implemented for data collection in parts of mainland Tanzania. The app is being installed on mobile devices available in health facilities for surveillance data collection with the aim of replacing the use of USSD for case reporting. This is due to the relatively higher costs and connection time limit associated with the USSD system. The ubiquitous access to affordable smartphones and the rapid spread of internet connectivity in Tanzania will facilitate a smooth transition to the custom android app for data collection throughout the country.
Multi-layer disease tracking and reporting: A coherent strategy for reducing the malaria burden in Tanzania
Within the past decade, the WHO released operational manuals for malaria surveillance to provide guidance to country settings that are in the control and/or elimination phases. The goal was to utilize all opportunities and resources in the control phase to minimize malaria incidence and mortality as rapidly and cost-effectively as possible. These guidelines, which were integrated into the MoH National Malaria Strategic Plan 2014-2020, informed the roll-out and large-scale implementation of the eIDSR in Mainland Tanzania. The platform is used by the NMCP to monitor malaria trends and accurately detect sudden increases in malaria incidence in a timely manner across multiple levels. The eIDSR and the country’s HMIS, based on the DHIS2 platform, are the two main components of its surveillance platform, facilitating timely and efficient malaria surveillance in line with the NMCP goals.
Using this platform, data is collected at the community and healthcare facility levels and subsequently passed up the healthcare management hierarchy from the council level to the national level for investigation, verification, analyses, resource mobilization and responses. The eIDSR server is configured with set varying thresholds for malaria cases in different settlements depending on the historical data. Where such historical data were absent, a three-week rolling average, as recommended by WHO, was used to set the threshold. The server would automatically notify relevant stakeholders via SMS whenever the threshold is crossed, prompting a timely response.
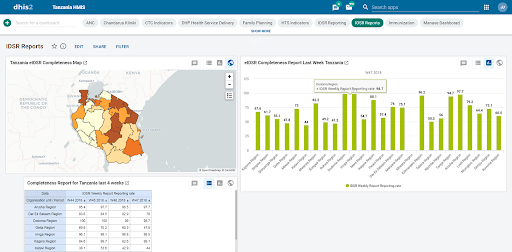
The NMCP, in 2013, launched weekly and monthly electronic reporting platforms using DHIS2 in Mainland Tanzania to support malaria burden reduction efforts and the transition from malaria control to sub-national elimination. The combination of annualized weekly eIDSR and monthly DHIS2 reporting completeness, malaria cases, and high incidence detection in areas with very low malaria density shows that the eIDSR is a useful tool for early outbreak detection, and the platform could be reliably expanded by adding more indicators and modules for case-based surveillance in very low disease density settings. These have had significant impacts on data completeness and quality which guide policy decisions. After weekly eIDSR reporting was implemented across the country, overall reporting completeness has gone from 90.2% in 2020 and 93.9% in 2021. Also, the proportion of weekly eIDSR testing increased from 87.0% in 2013 to 99.2% in 2021.
According to an expert analysis of the time trends of reporting, evaluating, test positivity, and malaria cases between 2013 and 2021, and weekly reporting of the mobile-powered eIDSR completeness in public and private health facilities have steadily improved over time. In 2014, the overall data completion rate was 51.1%. Since then, the completion rate has risen to 66.6% in 2018, 90% in 2020 and 93.9% in 2021. Similarly, timely reporting in areas of low and high malaria prevalence has gone from 8.7% and 9.2% in 2014 to 78.7% and 47.8% by 2018 respectively. Furthermore, comparisons of annual reporting completeness, malaria cases, and estimated annual incidence by malaria epidemiological strata revealed a higher parasite prevalence in 2020 and 2021 for both weekly eIDSR and monthly DHIS2 data. This highlights that quality surveillance data provided by the eIDSR and DHIS2 platforms has helped the MoH to better target malaria testing, thereby increasing the positivity rate.
These robust malaria surveillance systems aid NMCP in strategic decision-making, including more effectively targeting interventions as they progress towards elimination and preventing the re-establishment of transmission in areas where malaria has already been eliminated. An example of these interventions includes improved access to malaria diagnosis by microscopy and RDTs, made possible through reliable data from the eIDSR.
Improved data quality and trust, high malaria test yield for effective treatment and decentralized data availability
Reporting completeness and timeliness have improved significantly since the establishment of electronic reporting platforms while the overall national case incidences have reduced by 2.8% between 2017 and 2020. This progress can largely be attributed to the implementation of the eIDSR in conjunction with the adoption of the WHO malaria diagnosis and treatment guidelines, which promotes the testing of all suspected malaria cases and improves access to malaria testing through the widespread availability of malaria RDTs.
Based on data from the weekly eIDSR and monthly DHIS2 reporting, the proportion of confirmed malaria cases nationally has increased significantly, while the proportion of clinical cases treated presumptively has decreased from 30% in 2015 to 0.8% in 2021. This suggests increased positive cases yield from targeted testing due to good quality surveillance data. Also, there is now greater certainty about the accuracy of the reported malaria incidence rates throughout the country, which will accelerate the country’s progress to malaria elimination.
Furthermore, the eIDSR has contributed to a general improvement in IDSR data quality through the validation process that occurs at lower levels before surveillance data is sent to DHIS2. Additionally, the system facilitates early outbreak detection and notification for other diseases beyond malaria. This was observed in 2015 when national-level notifications of the cholera outbreak in Tanzania from the sub-national levels were sent through the eIDSR.
Finally, the eIDSR and DHIS2 HMIS systems have decentralized disease surveillance data access, analysis and use at all levels of healthcare management in Tanzania. This contributes to increased data use for policy formulation, intervention planning and monitoring, thereby helping the MoH advance its malaria eradication goals and achieve other healthcare targets.
Share your comments and questions about this project on the DHIS2 Community of Practice.