Optimizing access to HPV vaccination in Kenya by using data triangulation in DHIS2 to identify coverage gaps
The Kenyan National Vaccines and Immunization Programme and the Clinton Health Access Initiative adopted data-driven strategies to identify nearly 600,000 missed opportunities for HPV vaccination and increase the nationwide coverage rate from 13% to 63%
Cervical cancer is the fourth leading cause of death among women, and low-and-middle-income countries (LMICs) account for 90% of the global total of reported cervical cancer cases and deaths. Persistent infection with the human papillomavirus (HPV) is a known cause of cervical cancer. Fortunately, HPV infection can be prevented through the safe administration of the HPV vaccine in age-eligible adolescent girls. However, only 15% of age-eligible adolescent females worldwide had received their HPV vaccinations as of 2019.
With about 3,400 deaths per year, cervical cancer is the most common reason for cancer-related mortality in Kenyan women. In response to this, the government of Kenya introduced two-dose HPV vaccination into the routine immunization schedule, targeting 10-14-year-old girls through facility-based delivery in compliance with the WHO’s recommendations. Using triangulated hospital attendance and vaccination data in DHIS2, the team from the National Vaccines and Immunization Programme (NVIP) and the Clinton Health Access Initiative (CHAI) Kenya were able to leverage DHIS2 for data triangulation to identify nearly 600,000 missed opportunities nationwide during routine hospital visits. This information was used to boost the national HPV vaccination coverage from 13% to 63%. Subsequently, the team piloted a targeted HPV vaccination in 14 public healthcare facilities, observing a 49% increase in HPV coverage in those facilities. Plans are underway to implement this strategy nationwide, anticipating a marked increase in coverage.
“By leveraging technology solutions such as DHIS2, the decision-making process in public health can be enhanced, leading to more effective interventions and policies. Regular exploration and utilization of DHIS2 data enable informed and insightful decisions to improve public health outcomes.”
Leveraging data from DHIS2 and other sources to map and plug vaccination coverage gaps
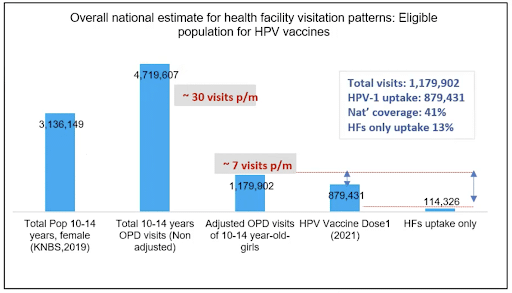
When the MoH in Kenya initiated the facility-based HPV vaccination strategy as a part of routine immunizations, the set target was to vaccinate up to 70% of all eligible young girls in the country. This number was estimated at 3.1 million girls. By the end of 2021, the HPV vaccination coverage rate stood at 13%, a far cry from the target set by the Ministry of Health. Health managers believed that this may be attributable to low hospital visits by the target population. To bolster the numbers, vaccination outreach activities were periodically carried out at schools. This approach was limited by inadequate funding, as school outreach is more costly than facility-based vaccination.
To figure out a more effective strategy for achieving the government’s objectives, the MoH and CHAI team decided to look for additional opportunities for increased vaccinations that were not obvious at the time. Consequently, they turned to data and DHIS2. The team started by examining the frequency of hospital visits by girls in the target population. To this end, outpatient data, immunization data, facility workload data – all of which are hosted in DHIS2 – and population data from Kenya National Bureau of Statistics were triangulated and analyzed to map the frequency of hospital visits by 10 – 14-year-old girls in the country.
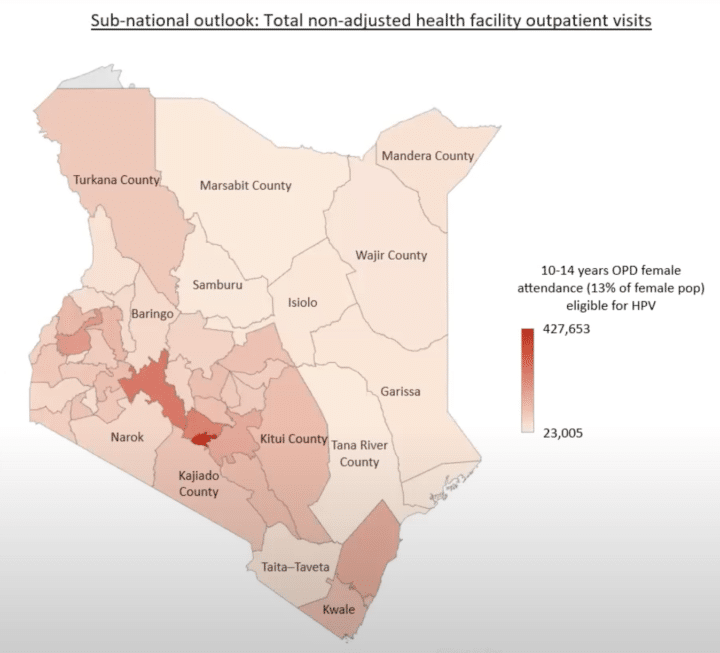
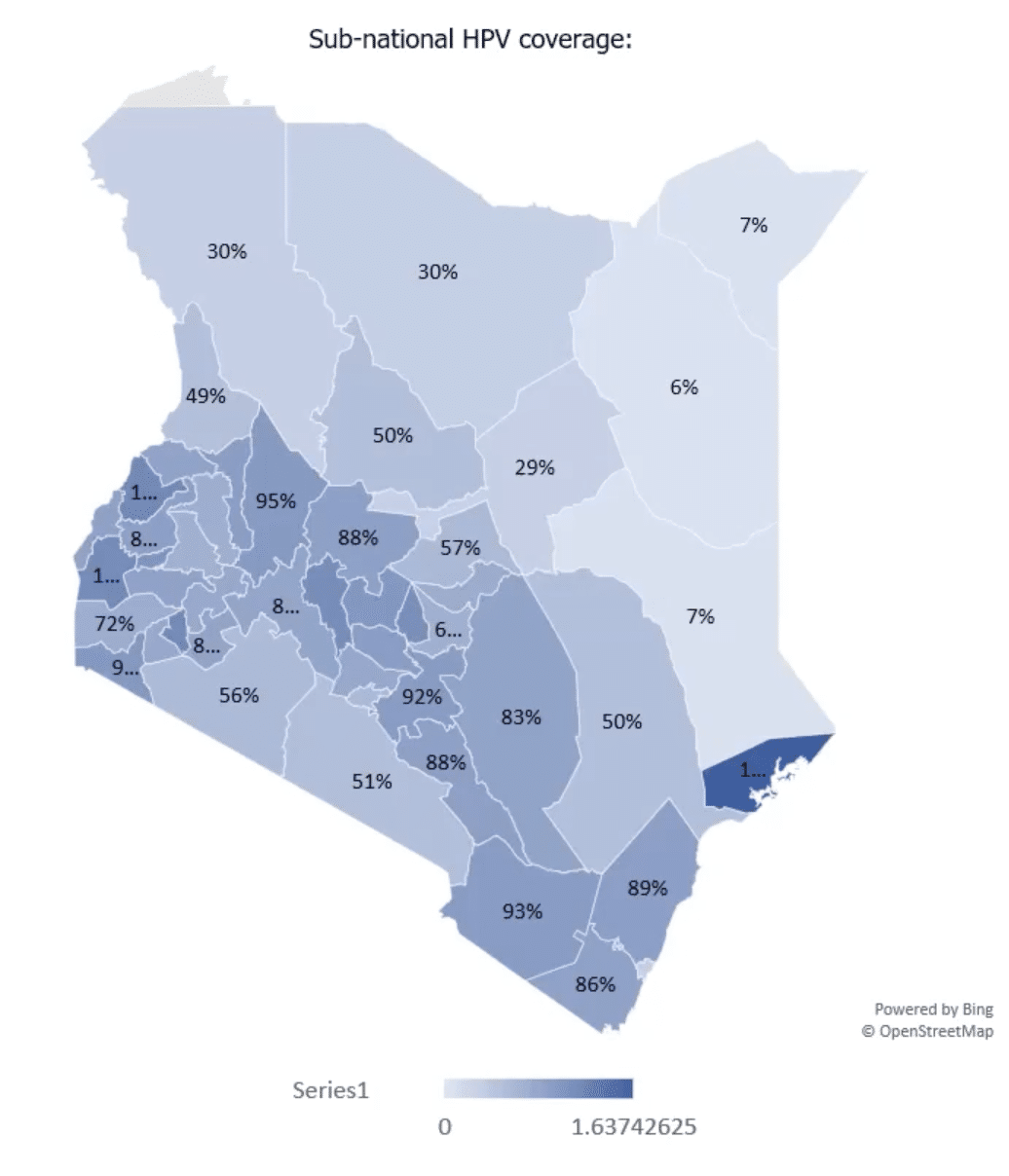
The team established the number of individual visits by reviewing the triangulated data in selected health facilities. After measures were taken to account for multiple visits to the same facilities or single visits to multiple facilities, the team conducted descriptive analysis and extrapolated the data to the different sub-national units as well as nationally. The analysis revealed that out of 1,179,902 individual visits to health facilities by age-eligible girls in 2021, of which 696,142 were potentially eligible for HPV vaccination, only 114,326 visits resulted in vaccinations. This leaves a gap of almost 600,000 eligible girls who visited the hospital but were not screened or vaccinated against HPV. Though the frequency of visits varied significantly across the sub-national units, this data provided good insights into missed opportunities, indicating that health facility screening can be leveraged in areas with high health facility visits to improve vaccination coverage.
By the last quarter of 2022, the vaccination rate was at 63% with a completion rate of 32%. However, despite financial constraints, the utilization of the DHIS2 platform opened up more strategies for accelerating and sustaining the HPV vaccination program in the country.
Strengthening health systems and targeting interventions using data-backed insights
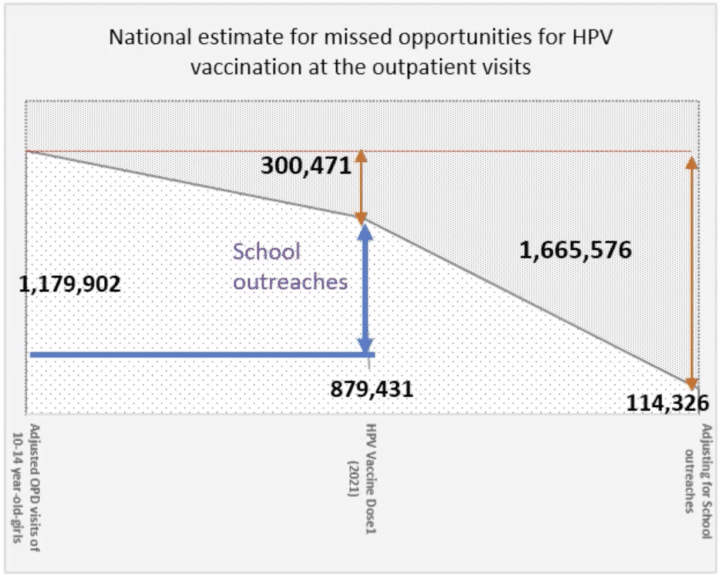
Following the findings from the data triangulation and analysis exercise on health facility attendance by the target population, the team opted to quantify the total missed opportunities for HPV vaccination by factoring in opportunities missed during school outreaches conducted during the same period. It was observed that the total number of girls who missed the opportunity to be screened and vaccinated for HPV throughout the country came to 1,665,576 in 2021. When compared to the total number of HPV vaccinations administered for the year, the adjusted missed opportunities were 581,816 eligible girls.
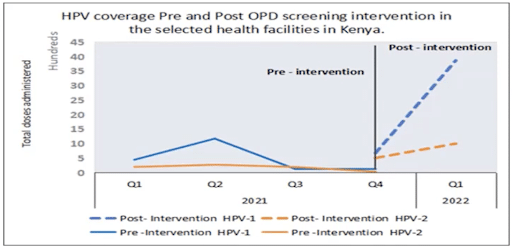
Using this data, a screening intervention was piloted in 14 public health facilities resulting in a 49% increase in HPV vaccination and demonstrating that data-driven targeted interventions could optimize vaccinations during health facility visits. Lessons from this DHIS2-supported data-backed intervention have inspired relevant health authorities in Kenya to initiate measures, such as a standardized vaccine screening tool, aimed at utilizing the opportunities presented by routine hospital visits to provide HPV and other essential vaccinations across the country, including routine immunization and COVID vaccines, and identify zero-dose children. Currently, the government has begun training healthcare providers to scale this strategy to other facilities throughout the country.
By addressing these missed opportunities from hospital visits and maximizing the potential of school-based outreaches, it is projected that there will be a significant enhancement in the coverage and effectiveness of the HPV vaccination program and help Kenya achieve the WHO target to eliminate cervical cancer by 2030.
This article is based on a presentation by Vincent O. Omondi of CHAI Inc., Kenya, at the 2023 DHIS2 Annual Conference. You can watch a recording on the DHIS2 YouTube channel.