Nepal employs DHIS2 Tracker for improved data and results in its national HIV program
Key stakeholders of the national HIV program in Nepal used biometric data in Tracker to enhance testing, care and treatment services, increasing the proportion of people receiving Antiretroviral Therapy (ART) from 65% to 84%
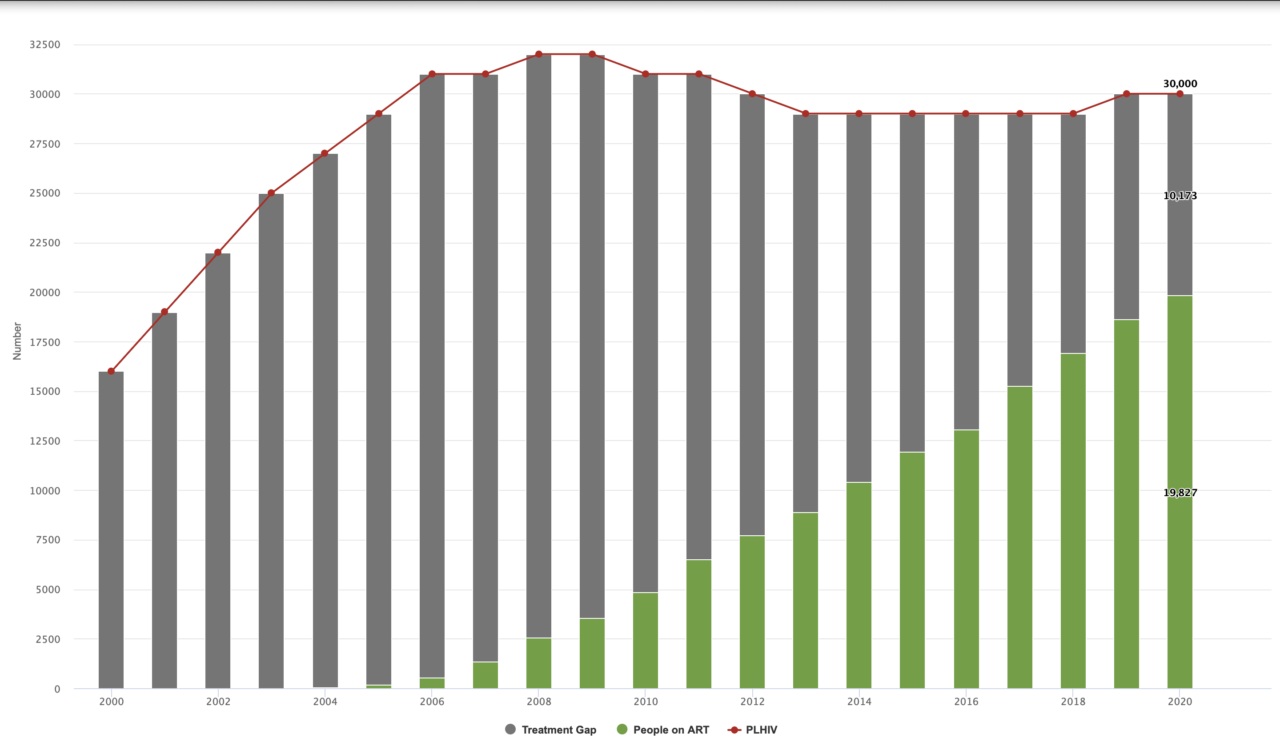
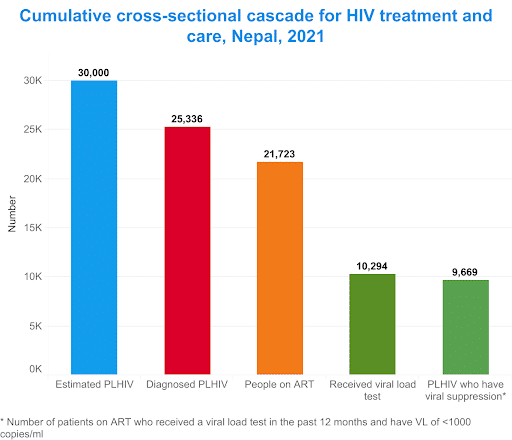
The first case of HIV in Nepal was reported in 1988. Though the prevalence of the virus in the country has remained low, at 0.13%, the total number of People Living with HIV (PLHIV) is estimated at 30,300 as of 2021. In 2017, the National Centre for AIDS & STD Control (NCASC) of the Ministry of Health and Population launched the HIV Care and ART Tracking System in Nepal. In the beginning, this DHIS2 Tracker-based information system received technical and financial support from Save the Children International / Global Fund programs and technical assistance from HISP India. The system is an innovative digital information system aimed at improving HIV care and treatment by providing seamless access to longitudinal data on all PLHIV who are enrolled in HIV services at all levels. The program uses biometric data to track PLHIV on antiretroviral therapy and across the continuum of HIV treatment, care and support, helping to ensure that PLHIV receive the necessary support and care to manage their condition effectively.
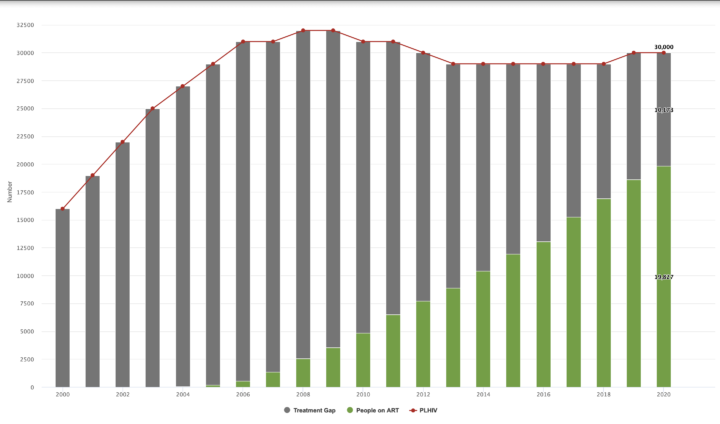
Since its launch, the HIV Tracker has had a significant impact on HIV care and treatment in Nepal. According to the NCASC, the HIV program and interventions have led to an increase in the number of people receiving HIV testing and counseling services, and an increase in the proportion of PLHIV receiving antiretroviral therapy (ART) from 65% in 2017 to 84% by 2021. The program has also helped to sustain good rates of retention in care among PLHIV throughout the country. This key indicator is tracked on a DHIS2 dashboard using data from the HIV Care and ART Tracking System. Furthermore, data from the system has helped program managers harmonize ART procurement planning, thereby improving logistics for HIV services. Overall, the program has been instrumental in improving the quality of care for people living with HIV in Nepal, and it serves as an important example of how innovative technology and approaches can be used to improve health outcomes.

Improving system efficiency and intervention planning by digitizing data collection using Tracker
There is no known cure for HIV. Because of this, individuals infected with HIV have to be in care and treatment all their lives. In Nepal, the existing paper-based HIV treatment registers were not effective at tracking cases through the care continuum due to inefficient management of unique identifiers, resulting in duplicate data, and over-estimation of indicators such as HIV treatment coverage rates. For example, when patients moved from one treatment site to another for care, they were sometimes enrolled into the program as new cases because it was difficult to search for their existing records on the paper registers. Furthermore, the paper-based system didn’t enable timely data analysis by program managers to help them estimate the effectiveness of interventions or programs. Finally, generating reports, including relatively simple ones such as “number of people currently on treatment” was slow and would often take weeks or months to complete, by which time, the actual figures have changed. These made intervention planning hectic, slow and in some cases, ineffective.
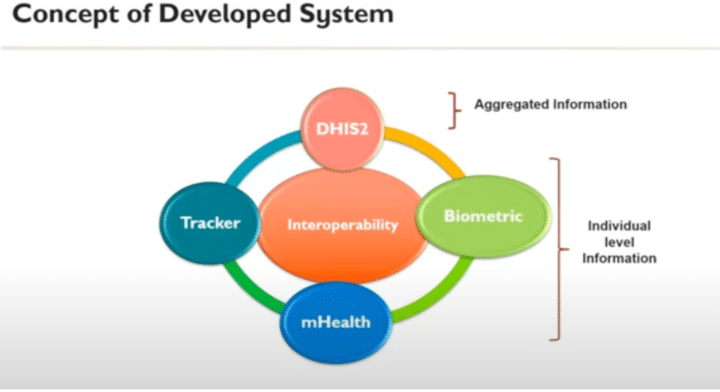
In response to these challenges, a patient-centered concept was developed that would prevent duplication of patient records, promote retention in care and provide easy access to individual-level data at all levels to facilitate program planning and help health workers offer custom care services to PLHIV based on their specific needs at any given time. This solution involved using Tracker to collect individual-level data; integrating DHIS2 with a biometric system for patient enrollment and verification; and interconnecting an existing mHealth system used to generate SMS notifications to PLHIV for improved retention in care. To implement this plan, the MoH collaborated extensively with HISP India which provided technical support for the program including Tracker customizations and server configurations (as outlined in the user manual).
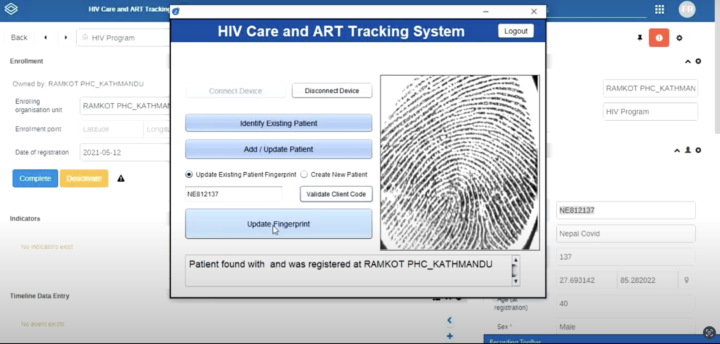
The biometric system is used to link new patients’ records to the Tracker app during enrollment and helps identify the medical history of existing clients. A two-part custom app was developed by HISP India to interconnect the biometric system with DHIS2: the client-side app was incorporated within the DHIS2 installation file; and the server-side app was hosted on a dedicated fingerprint server. Fingerprint readers are used to collect patients’ fingerprint data, which are verified, stored on the fingerprint server and then used to authenticate records in DHIS2.
The DHIS2 Tracker app, which facilitates registration and enrollment of new patients in the HIV program, is further leveraged for referring patients from HIV Testing and Counseling services to treatment services, including Antiretroviral Therapy (ART) services, as well as for follow-up visits. This allows the system to collect and catalog all patient data through all parts of the treatment and care continuum, making individual-level data easily accessible to program managers and healthcare providers at all levels. Using this information, treatment and information services are customized for individual clients, thereby achieving high retention in care and ultimately, viral suppression by reducing treatment gaps.
Additionally, the mHealth platform which was integrated with Tracker is used to generate SMS messages configured (and scheduled) in Tracker to consenting patients’ mobile phones in order to improve retention in care services. There are two types of messages sent to patients: appointment reminders, which include reminders for drug pick-ups, CD4, EID and Viral Load tests, among others; and general awareness messages aimed at improving overall health by promoting good health-seeking behaviors. Some general awareness messages help reinforce the importance of regular health check-ups, safe sex practices and other behaviors that would improve overall well-being.
The type and frequency of the text messages are applied to specific patients based on filters generated by custom scripts that run on the mHealth platform. All the messages are composed in the native Nepali language for easier understanding and better communication effectiveness. Furthermore, the SMSs are also formatted to promote confidentiality by using defined, unassociated terms to substitute the common ART treatment terms such as “PLHIV.” So far, these systems have helped sustain a trend of increasing retention in care, growing numbers of HIV-positive individuals enrolled in ART services and reducing stigmatization.
Implementation experience and lessons learned: Importance of user-centric approach to change management
The HIV care and ART tracking system in Nepal was implemented by NCASC, with the support of AIDS HealthCare Foundation, FHI360, Save the Children International and HISP India. After configuring the DHIS2 Tracker program in line with the country’s needs and objectives, the platform was piloted in three HIV treatment centers in Kathmandu, the capital of Nepal. Following the successful pilot, the implementation team developed a detailed user manual in the native Nepali and English languages to guide health workers who would use the system. Further to this, the MoH-led team procured, installed and customized all required infrastructure for the system, including servers and biometric devices. Subsequently, the HIV care and ART tracking system was rolled out in all HIV treatment centers incorporating feedback from users at the pilot sites. This was followed by training and onsite coaching to promote quick adoption of the system.
During the implementation of the HIV care and ART tracking system, some challenges were encountered, including the large volume of historical patient data to be entered into the Tracker platform. HIV treatment services started in Nepal in 2004/2005, but the DHIS2 Tracker system was piloted in 2017. This implies that about 13 years of backlog data needed to be transcribed into Tracker, resulting in an increased workload for site staff, especially in centers with already high client loads. Additionally, when HIV treatment services began in Nepal, records were created and updated using the Nepali Date format. After the Tracker platform was implemented with the Gregorian calendar, converting dates from the Nepali Date format was a significant challenge. Eventually, HISP India, NCASC and partners teams developed custom scripts and methods that accelerated the transcription process and eased the workload on healthcare workers.
There were also challenges in the uptake of the system as health workers who were already burdened by manual recording processes, did not understand why they were required to enter the same record on the new digital platform. As a result, many health workers were reluctant to use the system at first. To address this, stakeholder meetings were held with health workers to identify the cause of the disinterest by some sites. As explained by Dr. Keshab Deuba in his presentation at the Asia-Pacific Regional DHIS2 Conference, it was through these meetings that the team came to the realization that they had focused on the advantages of the platform to program administrators who would monitor real-time outcomes at the national level using individual data, but not enough on the benefits to the users at the health center level. In response, the team then educated end users on how the platform would ultimately reduce workload for them and support their day-to-day operations – like one-click monthly ART report generation in HMIS format and site-level dashboards that would help sites monitor aggregate and individual-level patient data – and how the ability to use the system to facilitate follow up with individual clients based on specific cases would improve retention, treatment, on-time pill pickup and virological suppression.
Another important user-focused initiative in the Tracker implementation in Nepal is the training video series developed by NCASC with the support of Save the Children International. These detailed and concise videos, recorded in the Nepali language using a demo version of Nepal’s HIV Tracker system, cover topics from logging into the system and updating user information using biometrics to enroll and update patient records, transferring patients to different facilities, documenting activities and generating reports. The video tutorials have become a vital resource to health workers in Nepal who can easily access guides for different components of the HIV care continuum, including testing, ART, EID and PMTCT services, thereby improving the capabilities of health workers to provide effective services to patients and helping ensure that the NCASC has the data it needs to monitor the HIV program as a whole. The development and sharing of training videos on YouTube proved to be immensely helpful during the COVID-19 pandemic as it enabled the capacity-building of health workers, which would have been difficult to achieve through in-person training due to the prevailing circumstances.
Finally, before Tracker was implemented for the HIV program, the team struggled to accurately calculate the type of regimen PLHIV were taking resulting in mismatches between the regimen type or drugs reported to logistics and the regimen reported in the monthly aggregated report of HMIS or to the M&E department. The use of DHIS2 Tracker has helped the team overcome these challenges. Different departments, including M&E and logistics, now jointly prepare a procurement plan based on Tracker data which accurately tracks the number of PLHIV and their regimen type and compares this with logistics supply and consumption reports. Any mismatch between the logistics report and M&E report can now be easily sorted out by reviewing the individual-level regimen-wise data recorded in DHIS2 Tracker or by contacting the health facility for confirmation by sending the client code. This has helped the team, not only in the procurement of drugs but also, in planning for viral load monitoring among PLHIV and identifying poor-performing clients via line list reports. In addition, supply stock-out information is also collected in Tracker from each HIV treatment site. Whenever a facility records a stock out of key HIV program commodities, this triggers an SMS sent to the mobile phones of logistics and M&E department officials, which facilitates immediate response by the team to coordinate a resupply.
In 2022, an integrated HIV care and ART tracking system was established to streamline all components of the HIV program, including prevention, testing, treatment, care, and support services. The objective was to consolidate data for the entire HIV continuum, ensuring a unified source for recording and reporting HIV-related data to the national HMIS. The system aimed to eliminate the vertical donor-specific information system and promote the use of a single DHIS2 Tracker-based information system for recording individual-level data and reporting aggregated data to the national HMIS. The initiative also aimed to foster collaboration among healthcare workers from the federal to the provincial and health facility levels. Financial and technical support for this phase was provided by the AIDS Healthcare Foundation, Save the Children International / Global Fund programs, and FHI360 through PEPFAR funding. HISP India provided technical support to ensure a smooth execution of this integration at the national level.
Resources for this story include the NCASC Users’ Manual for the HIV Care and ARV Tracking System and presentations by Dr Keshab Deuba at the DHIS2 Tracker Use Academy in 2021 and the Asia-Pacific Regional DHIS2 Conference in 2022.