Improving HIV Patient Follow-up in Liberia through Client-Level Electronic Data Management Using DHIS2 Tracker
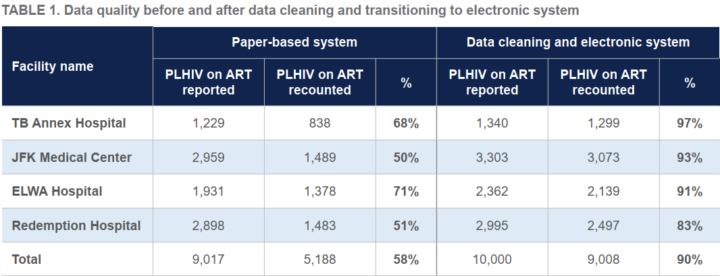
The PEPFAR- and USAID-funded EpiC project used DHIS2 Tracker to improve HIV management data accuracy from 58% to 90% in four Liberian high-volume facilities, helping ensure that up to 2,000 additional people received HIV care
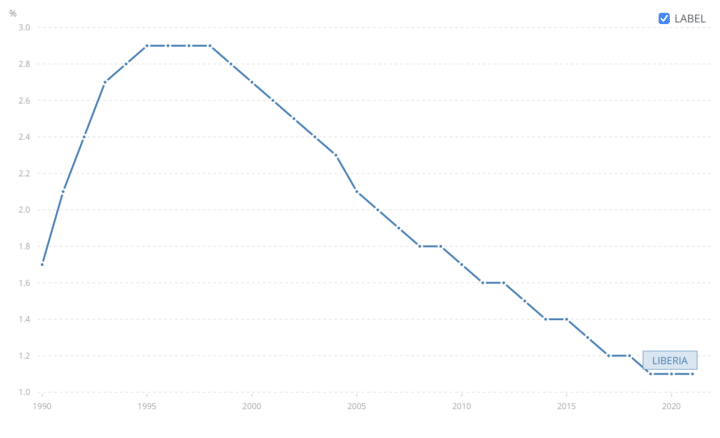
Historically, the prevalence of the HIV epidemic in Liberia has been relatively low when compared to other countries in the region, peaking at 2.9% in 1995. Since then, HIV prevalence in the country has declined steadily and now stands at an all-time low of 1.3% (2021 data) with a population of Persons Living with HIV/AIDS (PLHIV) at 35,000, of which 25,000 are on Antiretroviral Therapy (ART). Despite these remarkable achievements, Liberia still has a mixed epidemic with significantly higher prevalence rates among key populations such as sex workers, miners, transport workers, uniformed service personnel and mobile traders. A retrospective study of the HIV epidemic in Liberia for the period between 2014 and 2019, found that after 24 months, 41.8% of PLHIV in the country are lost to follow-up (LTFU). This high LTFU rate, among other factors, has impeded Liberia’s success towards achieving the UNAIDS 95-95-95 strategy which the country adopted in its National Strategic Plan (2021 – 2025).
In support of measures to achieve the global UNAIDS targets, PEPFAR and USAID funded the Meeting Targets and Maintaining Epidemic Control (EpiC) project in April 2019. The project, led by FHI 360, aims to achieve HIV epidemic control in multiple countries by improving HIV case finding, prevention, treatment programming and viral-load suppression. In 2021, EpiC partnered with the National AIDS and STI Control Program (NACP) in Liberia to implement the DHIS2 Tracker client-level data system to record and report HIV client information in 21 PEPFAR treatment sites, replacing the paper-based registers previously in use. These sites cover 70% of the entire country’s PLHIV who are on treatment. Since the successful implantation, HIV data quality in the PEPFAR-supported facilities has improved significantly from 58% to 90% in the top four high-volume facilities. The system has also helped program managers correct some miscategorizations of clients as active or non-active on treatment, including those who were erroneously attributed as deceased in the old system. This has helped ensure that nearly 2,000 people who were previously not accurately tracked in the HIV treatment system gained access to care.
The success of EpiC’s Tracker implementation has inspired the Liberian Ministry of Health and the Department of Defense to adopt Tracker for HIV data management in other non-PEPFAR-supported facilities throughout the country. Similarly, Plan International, a global Non-Governmental Organization focusing on the rights, security and welfare of children, has also implemented Tracker for its Key Population program in Liberia, drawing lessons from the EpiC project.
Reaching the last mile of the HIV treatment cascade through granular data analysis and improved data use.
The basic tenets of the UNAIDS 95-95-95 treatment strategy for tackling the HIV pandemic are to ensure that 95% of PLHIV know their status; 95% of those who know they are living with HIV are on ART; and 95% of those on treatment achieve viral suppression. This requires HIV program managers at all levels to make effective program guidance decisions using up-to-date and accurate data. In Liberia, since the HIV program was initiated in the 1990s, data management has been handled using paper-based registers and forms. In some cases, these forms and registers were not harmonized among different facilities, resulting in disjointed and fragmented data. This presented data quality challenges to the Ministry of Health as well as other HIV program partners in the country, especially in remote health facilities. In one example, the lack of standardized tools for data collection at all the HIV treatment sites nationwide hampered data retrieval and use, leading to uncoordinated provider/peer-led ART dispensing. In some cases, ART drugs were delivered to clients’ homes without documentation and for some without being registered. These practices limited access to quality data needed to facilitate granular data analysis and use for improved service provision, resulting in a 33% treatment gap.
Following the successful implementation of Tracker for client-level HIV data management in the 21 PEPFAR-supported facilities in Liberia, there was a notable improvement in data quality, patient retention on care and the quality of services delivered. In Q2 2022, 3660 clients were reported to have Interruption In Treatment (IIT), including 3,125 LTFU; 361 deceased; and 174 stopped treatment. A comparative analysis conducted in Q2 2023 showed that these figures have improved to 1,686 LTFU; 68 deceased; and 19 stopped treatment. This improvement is attributed to the proper classification of clients due to improved data in DHIS2, and the use of data to facilitate a case-based approach to managing clients and follow-up to improve services and prevent treatment interruption. The improved data quality has also supported targeted efforts by the program managers to reach the last mile with testing and treatment services in line with the strategic plan.
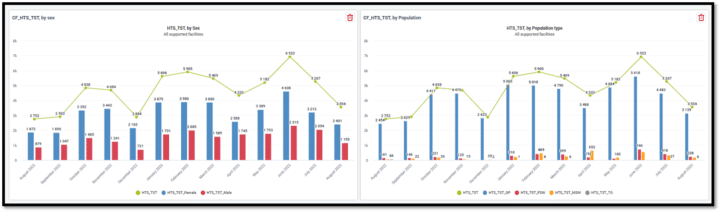
Furthermore, custom visualizations in DHIS2 which track essential indicators across the care continuum have provided health managers in the country with critical data for planning. Tracking of monthly data, visualized in DHIS2, supports efforts to target interventions aimed at reaching specific at-risk individuals, groups and key populations. This is further supported by the ability to disaggregate service delivery data by different categories for more granular analysis and insights.
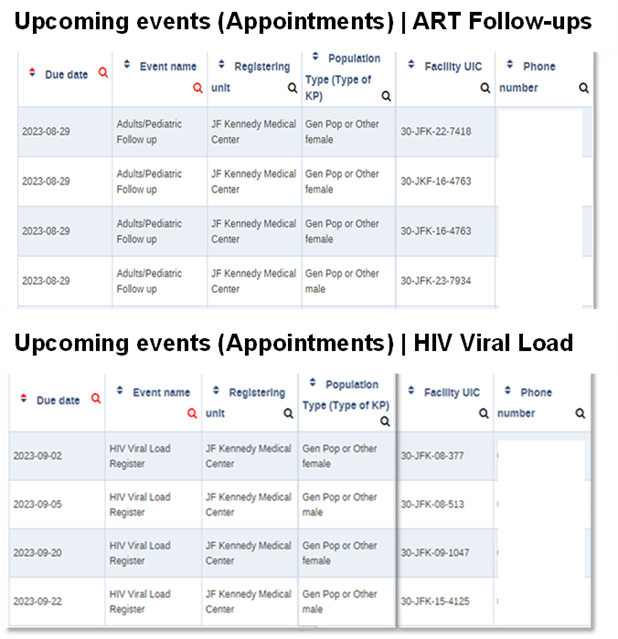
The Tracker system also provides line lists of clients due for ART refills or eligible for viral load tests and those who missed ART appointments. These lists are routinely used by providers and case managers to carry out quick corrective actions such as follow-up, treatment re-initiation, viral load testing and preparation of needed supplies and commodities as needed, thereby sustaining a high rate of retention on care services.
Adopting a systematic framework for the transition from paper-based to electronic HIV data management
EpiC, in collaboration with departments of the MoH, adopted the Exploratory, Preparatory, Implementation and Sustainment (EPIS) strategy in transitioning from the inefficient paper-based system to Tracker for HIV client-level data management. This standardized strategy helped the program implementing teams adopt a methodical approach to implementing Tracker. The process started with a needs assessment, during the Exploratory Stage, to establish the availability of requisite infrastructure including electricity, internet coverage and ART storage facilities. The team also held engagement meetings with stakeholders from the MoH, NACP and facility leadership to improve awareness and promote stakeholder buy-in towards ownership. To conclude this stage of the EPIS strategy, the team conducted Data Quality Assessment (DQA) at the four high-volume facilities to establish the documentation gaps and establish data quality baseline for future assessment.
Subsequently, in the Preparatory stage, the team recruited data entry clerks and procured materials and equipment necessary to mitigate potential challenges identified during the Exploratory stage. These included portable power generators, solar panels, client files, cabinets, computers, Android tablets, and internet devices for data entry. This was followed by the development of a data entry plan, categorizing the facilities into small, medium and high-volume based on the number of clients receiving ART services in each facility after which data entry clerks were trained on how to enter data in DHIS2. Finally, in this stage, the team conducted data cleaning exercises in the four high-volume facilities to organize and update the fragmented records.
In the Implementation stage, the transcription of the cleaned data from the paper registers into DHIS2 by the data entry clerks began. Data entry started with the small facilities and progressed to the larger facilities. The team further organized, filed, and stored client charts using unique identifier codes and conducted routine monitoring and support visits to ensure successful implementation. In total, 91% of all HIV management records in the 21 facilities previously held in the paper-based registers were successfully transferred into the DHIS2 Tracker.
Finally, in the Sustainment stage, the MoH developed a plan to migrate the data from the EpiC DHIS2 cloud server to the locally owned and managed MoH server. This supports the MoH’s decision to roll out this system in phases to the remaining 900+ non-PEPFAR facilities across Liberia, and will promote ownership as well as build the capacity of the Liberian MoH to independently sustain the DHIS2 server in the long run without donor funding, in line with the country’s Health Information Systems Strategic Plan.
This article is based on a presentation by Rachel Lyimo of EpiC / FHI360 Liberia at the 2023 DHIS2 Annual Conference. You can watch a recording on the DHIS2 YouTube channel.