Nigeria integrates last-mile vaccine supply chain data in DHIS2 to improve visibility and use at sub-national levels
The Nigerian Ministry of Health extended its DHIS2-based HMIS to include logistics and stock management for immunization programs, supporting improvements in vaccination coverage and a 98% reduction in reported stockouts nationwide
Every year, vaccine-preventable diseases such as diphtheria, tetanus and polio affect over 30 million children under the age of five years in Africa, resulting in an estimated 500,000 deaths (WHO). Nigeria alone accounts for approximately 30% of zero-dose children worldwide, causing high child mortality rates. Nigeria has made concerted efforts to reduce child mortality through routine vaccination programs carried out in all Primary Healthcare Centers (PHCs) in the country. These are complemented by targeted immunization campaigns that focus on specific diseases such as polio and meningitis in communities with the lowest coverage.
In its bid to strengthen immunization systems in the country and further achieve national healthcare objectives, the Nigerian MoH developed the Nigerian Routine Immunization Strategic Plan (NRISP) 2013 – 2015, which provided a strategic framework for achieving the goal “to reduce the number of unimmunized children by attaining at least 87% sustained national coverage with no fewer than 90% of the Local Government Areas (LGAs) reach(ing) at least 80% of infants with all scheduled antigens by 2015.” The policy identified factors that hinder successful immunization programs in Nigeria including ineffective supply chain and logistics, poor service delivery and poor data quality.
In recognition of these challenges, the MoH–with funding from the CDC and technical support from HISP Nigeria–has taken steps to improve immunization logistics by implementing a unified system for quality data collection and analysis using DHIS2. This initiative integrates immunization logistics data management with the existing DHIS2-based national HMIS as a single source of health data for policymaking and program planning. The unified system has improved the transmission of vaccine stock data and cold-chain equipment status directly from PHCs, enhancing last-mile visibility and facilitating timely decision-making for better outcomes, which–among many other factors and interventions–contributed to a The Nigerian Ministry of Health extended its HMIS to include logistics and stock management for immunization programs by implementing a unified national reporting system in DHIS2 resulting in a 98% reduction in reported stockouts nationwide from 2014 to 2021 using the DHIS2 platform.
“Now, at a glance, we know the number of vaccines used, where the gaps are and how to channel the vaccines to where they are most needed.”
Jirgi Hosea B – State HMIS Officer, Kaduna State, MoH Nigeria
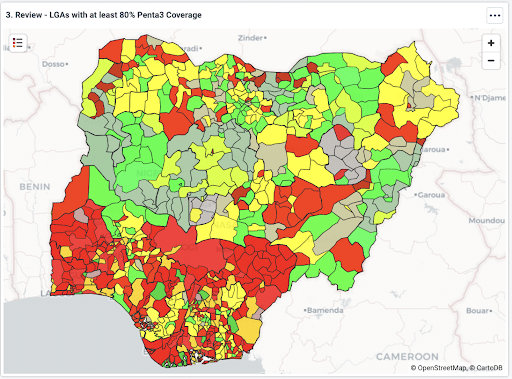
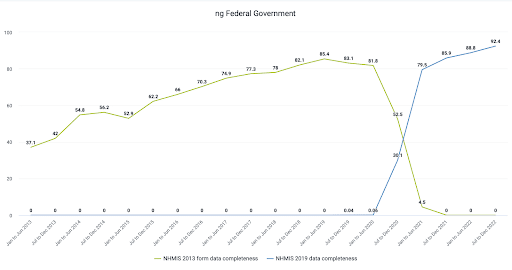
To ensure the availability of good quality data for better data-backed decisions, the MoH set a target of 95% for data completeness and timeliness of reporting. In 2013, before DHIS2 was implemented, data completeness averaged 40%. Since the DHIS2 platform was implemented in 2014, this indicator has improved remarkably to 93.1% at the end of December 2022. Likewise, the system has helped improve vaccine coverage, especially for the most important antigens in the country. For example, the 2021 Multi-Indicator Cluster Survey reports that Penta3 coverage has grown from 33% in 2016 to 57% at the end of 2021. While still below national targets, this represents a significant and sustained improvement over time.
Integrating routine immunization data in DHIS2 for improved efficiency and data quality
Unavailability of good quality data, especially at the LGA and health facility levels, impedes effective decision-making for immunization programs. Prior to the introduction of DHIS2, immunization service data was collected on paper registers in health facilities and transmitted via paper-based Monthly Summary Forms (MSF). Usually, designated facility staff would extract immunization data from the registers by manually counting and entering these totals into the MSF which was forwarded to the LGAs at the end of the month. The LGAs would collate data on paper from multiple facilities within their area of responsibility and forward them to the state levels where further aggregation was done before they were entered into the National HMIS (NHMIS). This process was fraught with data quality challenges including incomplete data and delayed reporting.
HMIS health data is used for policy formulation, monitoring and evaluation, so data quality issues pose a significant challenge for effective governance. To address this, in the first quarter of each year, the MoH conducts a national data quality self-assessment to measure the reliability of national health data. While the pre-DHIS2 assessment carried out in 2012 showed that 98% of data reporting the coverage for all antigens for immunization programs were accurate, significant gaps in data completeness were identified. A subsequent WHO evaluation found that “only 36% of health facilities recorded prior doses of DPT in registers, and only 56% (of the facilities) updated their registers with information from a child’s immunization card.” This implied that more data was available on the individual immunization cards which parents take home than on the facility-based paper registers. A disconnect in data flow and feedback between the facilities and the LGAs was also observed in this paper-based system.
In 2013, the National Council on Health (NCH) adopted the DHIS2 platform as a unified electronic NHMIS system to achieve a single source for healthcare data. In line with this directive, the digitization of data collection systems for immunization programs using DHIS2 to improve data quality and availability was initiated by the MoH with funding from the CDC through the National Stop Transmission of Polio (NSTOP) program. In 2014, a pilot of the DHIS2 Routine Immunization (RI) module was implemented in Kano, northwest Nigeria, and was subsequently rolled out across the country, reaching national scale in 2017.
Improving effectiveness in Nigeria’s immunization systems by integrating logistics data into DHIS2
An efficient logistics system, including reliable cold-chain infrastructure, is critical to the success of immunization programs. Many vaccines must be stored within specific bands of temperature ranges to remain efficacious. In Nigeria, inadequate supply and cold chain infrastructure, worsened by an unreliable power supply, contribute to logistical challenges resulting in vaccine stock-outs and wastage. In 2012, a Cold Chain Assessment conducted as part of the periodic Vaccine Audit by the MoH showed that 43% of cold chain equipment (CCE) at the LGA and facility levels was non-functional. Furthermore, the study also found that 96% of the health facilities visited had no refrigerators for vaccine storage, severely limiting vaccine inventory capacity in those facilities.
Consequently, the NRISP prioritized logistics as the number one factor for improving national routine and targeted immunization programs from 2013 and beyond. Its logistics objective is to “guarantee 100% adequacy of bundled quality vaccines for safe immunization at all times.” The MoH planned to achieve this by increasing sub-national level cold chain infrastructure functionality from 47% to 80%. In order to collect and monitor cold chain and immunization stock data, Nigeria’s MoH turned to DHIS2. Following the successful testing and implementation of the Routine Immunization module described above, the development, training and nationwide rollout of the DHIS2-integrated immunization logistics forms commenced in 2017.
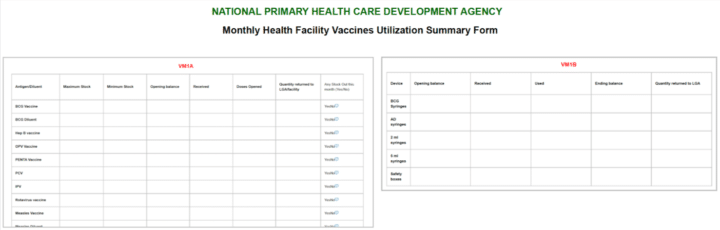
The digitization process, which was implemented by the African Field Epidemiology Network (AFENET) with technical assistance from HISP Nigeria, started with the development of supplementary datasets for the MSF to cover logistics and newly introduced routine immunization antigens. The supplemental datasets are grouped into two, namely: VM1A which collects data on the stock situation for all antigens and discarded doses; and VM1B for syringes stocks data and monthly devices status reports. The expanded MSF replaced the older reporting form and was also incorporated into the NHMIS already hosted in DHIS2.
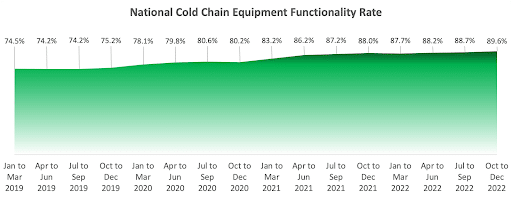
Subsequently, some health facilities were provided with mobile devices and internet connectivity to report directly into the national repository while data collected manually on the MSF in facilities without internet services are collated and subsequently entered into the NHMIS at the LGA level. Data entered in DHIS2 is available electronically at the national and sub-national levels, including in the facilities, supporting last-mile visibility. Since 2019, an average of 9,000 facilities have been reporting immunization logistics data on mobile devices while plans are on to extend this capability to all health facilities in the future. Leveraging improved data available in DHIS2 and partner support, the MoH has been able to exceed their performance target and achieve a cold chain infrastructure functionality rate of almost 90% by December 2022.
Data use for immunization program planning: Triangulation of stock data and other indications using publicly accessible custom dashboards
An important feature of the integrated HMIS and immunization logistics data management system in Nigeria is the capability for close monitoring of key indicators using triangulated supply chain and service data, which supports timely decision-making. This has brought positive results. A review of data from Nigeria’s HMIS shows that the total stock-outs of vaccine supplies reported in 2021 was 626, down from a high of 31,687 vaccine stock-out reports in 2014, a 98% decrease. This progress has been facilitated by routine reporting from PHCs into DHIS2, combined with effective monitoring and timely action throughout the immunization program.
Using DHIS2, immunization program managers are able to visualize key indicators such as stock levels, doses administered and wastage. These help managers, particularly at the LGA level, better coordinate immunization logistics planning to minimize vaccine stock-outs across the country and achieve national immunization objectives. For example, when a health facility is out of vaccine stock and this is indicated on the dashboards, this triggers a redistribution from a neighboring facility with sufficient stock of the vaccine to boost immunization efforts.
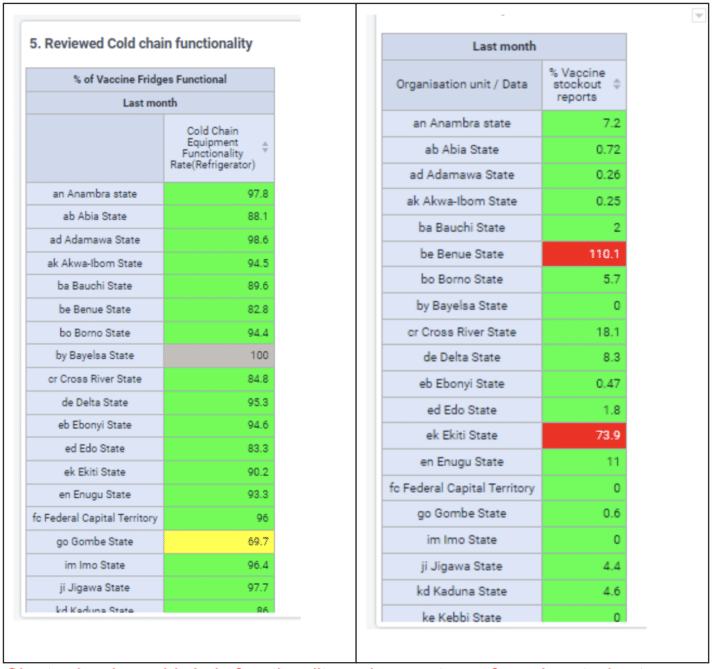
Furthermore, DHIS2 dashboards facilitate data triangulation, helping managers to compare supplied vaccines with administered doses. Where a disparity is observed, the RI teams can investigate, taking the wastages into account, and make recommendations. In addition, the DHIS2 platform enables program managers to monitor the operational status of cold-chain equipment up to the facility levels. Immunization logistics data collected on the MSF include relevant information about the availability and functional states of cold-chain equipment throughout the country to inform necessary actions for sustained functionality and reduced vaccine wastage.
Nigeria’s HMIS also supports data use more broadly. Essential indicators such as reporting rates, immunization coverage rates, stock levels and vaccine allocation are made available in user-friendly dashboards. Using these dashboards, field immunization workers, monitors and all healthcare staff in the country can access up-to-date data in various visualizations to support planning and timely actions. Specific protocols for necessary follow-up actions by specific groups of users have also been developed to facilitate immediate response when the needs arise, including in response to dashboard items that are color-coded using a green-yellow-red scorecard approach to give clear visual indications of potential issues to address. For example, when the indicators for the functional status of cold chain equipment turn from green to yellow indicating faulty equipment, the facility is expected to report this to the LGA level which would fix the defect quickly and report to the state level. If immediate repair of the equipment is not possible (in which case the indicator would be flagged red), the LGA will notify the State level officials or national program managers who would facilitate the replacement of the equipment. Also, the system keeps track of expected reports, reporting rates and timeliness to promote good quality data at all levels. The publicly accessible dashboard built in DHIS2 has become a tool for healthcare workers, students, and researchers to get up-to-date immunization data, thereby promoting data use.
Way forward: Integration of HMIS and OpenLMIS for last-mile data visibility
As more facilities are provided with internet services and mobile devices, the MoH hopes to achieve real-time monitoring of priority indicators for prompt actions by designated officials. In the future, the MoH plans to integrate the HMIS with OpenLMIS for facility-level stock and inventory management. This is aligned with the DHIS2-LMIS approach that leverages DHIS2 for last-mile stock data collection to support end-to-end supply chain management. When complete, this will facilitate better last-mile visibility of stock levels in all health facilities using DHIS2 in the country. Providing last-mile stock data, particularly consumption, can greatly improve the accuracy of forecasting and demand planning, greatly improving the efficiency of the supply chain and vaccine availability at the point of care. Lacking this consumption level data, forecasts are based on old or inaccurate data, or even worse previous quantities shipped, which inevitably leads to demand distortion1. This initiative is still in progress as of early 2023.
Watch a presentation on this system by HISP Nigeria at a DHIS2 for Immunization webinar on the DHIS2 YouTube channel