Improving reporting of morbidity and cause of death in Zimbabwe with DHIS2
An innovative solution developed by HISP Zimbabwe embeds ICD-11 coding directly in DHIS2 Tracker programs, improving data quality and facilitating automated reporting, providing health authorities with near real-time inpatient morbidity and mortality data for decision making.
High quality and timely inpatient morbidity and mortality data are critical for effective health system planning, disease surveillance, and evidence based policy development. In many low and middle income countries, inpatient reporting remains fragmented, largely manual, and dependent on outdated disease classification methods, limiting the availability and usability of clinical data for national decision making.
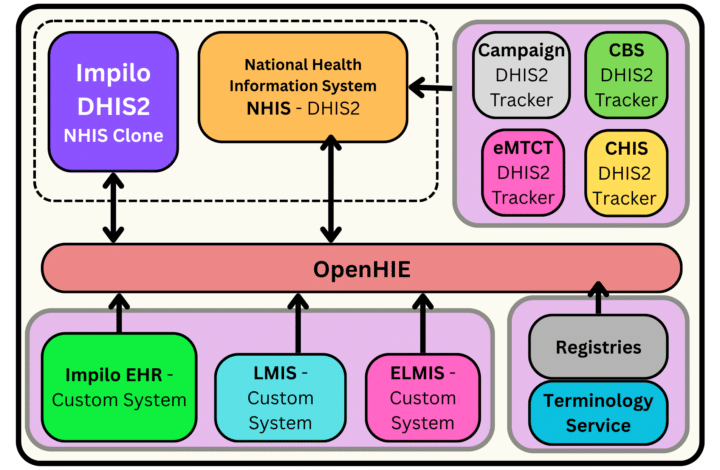
In Zimbabwe, inpatient data are captured through a Case-Based Surveillance (CBS) system built on DHIS2 using Event programs for individual-level data, while aggregated national health reporting is managed through the DHIS2-based National Health Information System (NHIS). While both of these systems have functioned well on their own, a lack of automated integration between them has made it difficult to incorporate CBS data into routine reports, delaying access to key morbidity and mortality insights.
To address this, Zimbabwe’s Ministry of Health and Child Care (MoHCC)–with financial support from The Global Fund, project management from HISP Africa, and technical support from HISP Zimbabwe–has worked to integrate these systems. A key element of the approach is semantic interoperability leveraging standardized ICD-11 codes for diagnosis and cause of death, featuring an innovative solution for embedding ICD-11 coding directly in DHIS2 data entry forms. This approach strengthens data quality, reduces manual reporting, and offers a scalable model for operationalizing ICD-11 coding in DHIS2.
Facilitating case-based to aggregate integration through semantic interoperability
A significant barrier to system integration is semantic interoperability. Different from technical interoperability, which is the ability of systems to “talk” to each other, semantic interoperability refers to the ability of systems to “speak the same language” by using the common terminology or codes, allowing data to be easily mapped and transferred between them.
A commonly used terminology standard in health systems is the ICD (International Classification of Diseases) code framework. ICD codes, which are defined and maintained by the World Health Organization (WHO), are standardized, alphanumeric medical identifiers used globally to classify diagnoses, symptoms, and causes of death. The use of ICD codes provides a common foundation for tracking public health trends, ensuring continuity of care, and facilitating national, regions, and global reporting using a shared framework.
The ICD code list has gone through several revisions over the years. In January 2022, ICD-11 was released to replace the previous generation, ICD-10, providing a much more granular level of coding to improve diagnosis accuracy and a fully digital code repository to replace the previous paper-based code list. The technical work of transitioning health systems from ICD-10 coding to ICD-11 also creates opportunities for improving system integration, though adoption of ICD-11 has been slow, with few low- and middle-income countries making the shift in the four years since its release.
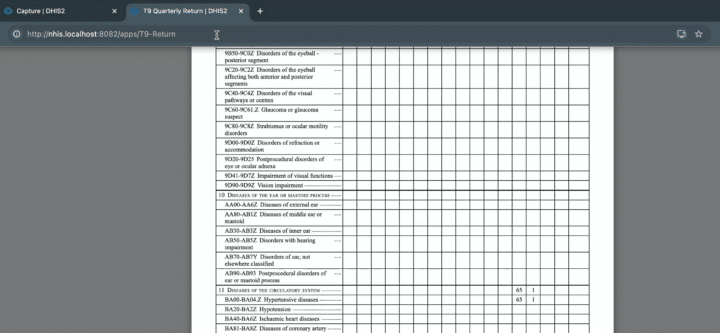
In Zimbabwe, the MOHCC’s CBS system has used ICD-10 coding to collect inpatient morbidity and mortality data. The ICD-10 codes were manually copied from a physical book and configured in DHIS2 Tracker programs as option sets, a cumbersome process which made updates difficult and posed challenges for integration between the CBS and NHIS systems. The previous configuration also limited the MOHCC’s ability to produce the T9 report, an aggregated report that tracks inpatient diseases, maternity conditions, admissions, and treatment outcomes.

In the process of upgrading the CBS to ICD-11, HISP Zimbabwe has helped the MOHCC implement a new approach that streamlines this integration, leveraging a centralized, reusable ICD-11 coding service to facilitate semantic interoperability and permit data exchange in near real time. They also updated the T9 report to reflect ICD-11 coding, providing the MOHCC with a complete overview of all relevant diseases and health outcomes, enabling them to monitor Zimbabwe’s population health more effectively.
Innovative technical approach to ICD-11 integration in DHIS2
Since the release of ICD-11, there have been some initiatives across the HISP network to help incorporate it into national health systems. One example was the Cause of Death app developed by HISP Vietnam, which successfully integrated ICD-11 coding into DHIS2 through a custom application. This app has also been implemented in other countries, such as Ghana, where it has been successfully adapted to meet the needs of the local context. However, this app was designed specifically for mortality data, which made it unsuitable for Zimbabwe’s data needs that also include morbidity surveillance.
In designing their local solution, HISP Zimbabwe decided to leverage a new functionality of the DHIS2 platform: Tracker plug-ins. This extensibility feature allows DHIS2 system owners to develop customized components that can be inserted into standard Tracker programs in DHIS2, without the need to develop and maintain an entirely separate application.
The plug-in developed by HISP Zimbabwe supports the creation of data entry fields that draw directly on ICD-11 search and validation services, enabling real time diagnosis and cause of death coding without the need to store ICD-11 codes as option sets within DHIS2 itself. This is particularly important for the transition from ICD-10 to ICD-11, as the total number of ICD codes has increased from around 8,000 to over 55,000 between these two versions.
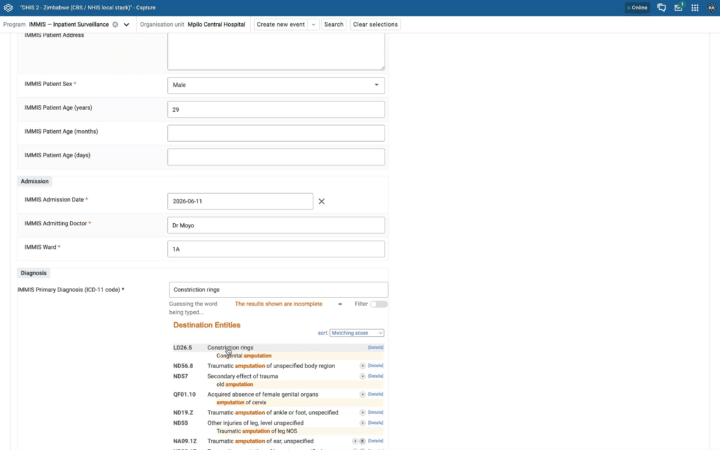
Using this plugin, the “diagnosis” data entry field in the CBS pulls directly from the WHO ICD-11 coding tool. This lets the health worker select or search for the appropriate disease name from the ICD-11 list within an interactive widget that takes advantage of ICD-11’s built-in natural language processing for an optimized “smart search” experience. When an item is selected, a pop-up window in DHIS2 shows the disease name, ICD-11 code, subcategories, and extensions. Additional fields are included in the data entry form for secondary and tertiary diagnoses. If the patient outcome is deceased, the “cause of death” field will also pull the ICD-11 codes so that the correct cause of death can be recorded. If the health worker is not sure which code is correct, they can click a button in DHIS2 to be taken directly to the ICD-11 coding site for more information to help input the correct diagnosis.
“Now you can have any Tracker program using the standard Tracker package, and if you want to use ICD-11 you just create an ICD-11 field… This is much more innovative than we thought.”
— Bob Jolliffe, DHIS2 Integration Team, HISP UiO
This configuration also supports automated migration from ICD-10 to ICD-11 for legacy data and smooth transitions for future upgrades to ICD-11. Thanks to the Tracker-Aggregate integration implemented by HISP Zimbabwe, patient data that has been entered in the CBS is automatically transformed into anonymized indicators that are sent to the NHIS in near real-time. In the NHIS, a summary of patient outcomes can now be seen on the T9 report, which is now organized according to ICD-11 chapters, with disaggregations for subcategories.
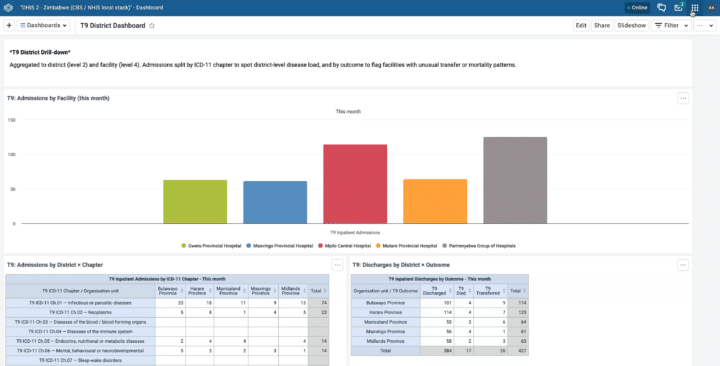
The solution also conforms to Zimbabwe’s standard Medical Certificate of Cause of Death format, supporting complete and accurate cause of death reporting. In addition, dashboards have been created in the NHIS showing data that has been aggregated from the CBS system, making it easier for health system stakeholders to monitor morbidity and mortality data in near real-time.
An underlying element of this integration that is significant is its use of Zimbabwe’s existing interoperability architecture beyond DHIS2. Instead of embedding the ICD-11 toolkit within individual applications, HISP Zimbabwe’s solution involves running the WHO ICD-11 repository as a central application hosted on Zimbabwe’s national data centre and leverages the Open Health Information Mediator (OpenHIM) to facilitate interaction between the ICD-11 service and the DHIS2 Tracker plug-in (and potentially other systems). This design promotes interoperability, reduces duplication of coding logic, and mitigates performance risks associated with managing large ICD-11 code sets within DHIS2. It is also flexible, and can be implemented with any suitable middleware, depending on local architecture and preferences.
An important contribution to DHIS2 role as lightweight EMR
The significance of this ICD-11 solution goes beyond Zimbabwe’s CBS system. In a number of countries, there is growing interest in leveraging DHIS2 as a lightweight Electronic Medical Record (EMR) system for primary health care. Like the CBS, these EMRs need to collect individual patient data and report it upward through the health system.
Any EMR, whether built on DHIS2 or another software system, needs to support standard terminologies such as ICD-11 in order to function effectively. Having a native solution for ICD-11 support in DHIS2 is a key component for the viability of DHIS2 as an EMR solution.
Next steps: Piloting and scaling in Zimbabwe & sharing with the global DHIS2 community
The process of designing and implementing this solution has been ongoing in Zimbabwe since 2025, with financial support from The Global Fund. As of June 2026, the solution is entering its final testing phases, to be followed by user acceptance testing and training. Barring any last-minute complications, the solution is expected to go live by the end of July 2026.
HISP Zimbabwe has developed capacity building plans, including SOPs and system documentation to support this rollout. However, the need for additional capacity building is expected to be minimal, as the solution is an extension of the MOH’s existing DHIS2 setup and infrastructure, making it easier for MOHCC personnel to take on and support this initiative.
While this project has been conceived and led by the MOHCC, and HISP Zimbabwe has been primarily responsible for the technical design and implementation, the development of the ICD-11 plugin has been supported by a continent-wide collaboration, with HISP groups and individuals in Malawi, Rwanda, Ethiopia, and West and Central Africa–and experts from WHO–participating in the evolution of its design. The HISP Africa continental hub has managed the Global Fund project that supported this work, while the DHIS2 integration team from HISP UiO contributed with technical input and facilitation support.
The Team from HISP Zimbabwe presented this work to the global DHIS2 community at the 2026 DHIS2 Annual Conference, helping to raise awareness about this approach among other countries that may be interested in implementing a similar solution locally. Ultimately, this ICD-11 Tracker plug-in will be published as a shared resource, available for any DHIS2 system worldwide to download and use.
Learn more about this project by HISP Zimbabwe: