The DHIS2 Annual Conference takes place from 15-18 June 2026! Learn more

The DHIS2 Annual Conference takes place from 15-18 June 2026! Learn more
As a native digital health registry, DHIS2 is a viable option for a lightweight EMR to support primary healthcare delivery. Explore the built-in features of DHIS2 that support facility-level collection and management of patient records and other longitudinal health data
There are a number of different approaches to collecting and managing health information on individual patients and clients. Before discussing the role of DHIS2 in this space, we will review some commonly used terms and discuss the purposes they serve and functionalities they each are intended to provide. In drafting the working definitions below, we have drawn on authoritative sources where possible, while acknowledging that the boundaries between these terms are not always clearly defined or universally agreed upon.
While best known as a platform for collecting and analyzing aggregated health data for population-level analysis and planning–as a Health Management Information System (HMIS) or national health data warehouse–DHIS2 is also widely used for managing individual-level patient and client data. Through DHIS2 Tracker programs, Ministries of Health and other organizations can easily collect and manage key information for individuals for one or more health programmes over time.
In the sections below, we explain how DHIS2 can be used as a digital registry, as a shared health record/EHR, and as a facility-level EMR for primary healthcare. It is important to note that due to the flexible, modular nature of DHIS2, these do not need to be thought of as separate systems–they can each be employed within the same national DHIS2 architecture, and deployed at different scales and in different geographies or contexts depending on the needs of the health system and the country’s readiness for individual-level data collection based on its DHIS2 maturity profile. This means that countries can use DHIS2 to begin collecting patient data in a limited way (such as for high-priority programmes or targeted districts) and then build up their system over time without the need to replace the underlying software platform.
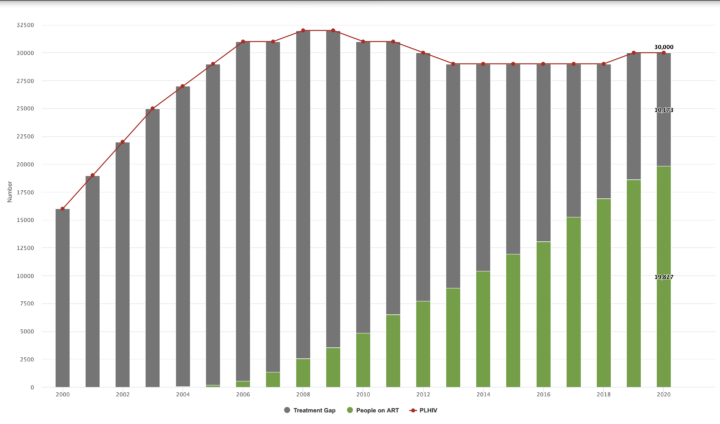
Digital registries built on DHIS2 have proven effective in achieving results for high-priority health interventions–such as helping to reduce vaccination dropout rates and improve TB surveillance and HIV treatment adherence. When implemented in DHIS2, these systems also benefit from several key EMR-like features–including decision support, automated patient messaging, and longitudinal records. Registries implemented in DHIS2 also benefit from robust features for automating the aggregation and analysis of individual-level data, allowing seamless integration with the HMIS for routine reporting and analysis of key indicators.
The use of DHIS2 as a digital registry is well established. DHIS2 is listed by GovStack as a Digital Registry “Building Block” software tool, supporting Digital Public Infrastructure (DPI) approaches for individual-level data management in the health sector and beyond. More than 80 countries around the world use DHIS2 to manage individual patient or client data for one or more health programmes, with hundreds of millions of individual records in DHIS2 systems worldwide. Some countries, such as Palestine and the Maldives, have combined numerous programme-specific Tracker modules together into one holistic system for electronic patient records in DHIS2.
By deploying DHIS2 as a Digital Registry/Tracker or lightweight EMR, countries can also leverage its robust data management and analysis features to use DHIS2 as a shared repository, which is supported by DHIS2’s default role as a centralized national registry. DHIS2 can also serve as an EHR/shared health record within a larger health information system architecture, allowing countries to bring together individual health records and data from a range of EMRs, including EMRs that are deployed using other software solutions. In scenarios where there are many kinds of EMRs/Trackers in use in one country, DHIS2 can thus provide a unified platform in which data from these siloed systems can be analyzed holistically–including linking individual patient data with routine health data in the national HMIS–providing health stakeholders with better oversight and ability to analyze and respond to health trends.
Using DHIS2 as a lightweight or “mini” EMR at primary care level offers several advantages – particularly in contexts where full EMRs are impractical due to cost or infrastructure limitations. Because such systems can be built within existing DHIS2 infrastructure–and because it is deployed as a multi-tenant system, with one central instance serving multiple health facilities, unlike EMR solutions that must be locally deployed at each facility–Ministries of Health can introduce longitudinal patient records and EMR-like functionalities at the point-of-care without the heavy costs and delays associated with deploying EMRs at scale. They also benefit from DHIS2’s proven design for low-resource settings—supporting offline mobile data capture and native aggregation of patient-level data into national systems. Moreover, DHIS2’s interoperability and extensibility allow for additional EMR features through custom apps or integration with other platforms.
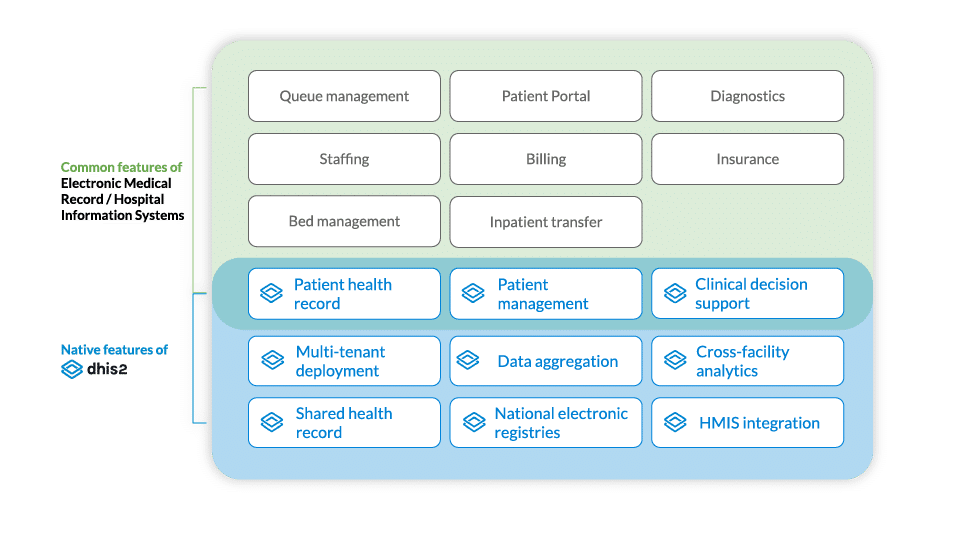
Despite these advantages, it should be noted that DHIS2 was not specifically designed to support the full range of EMR functionalities. It lacks key functionalities required by larger hospitals and inpatient facilities, such as billing, insurance, and diagnostic workflows; patient portals, appointments, and queueing; as well as staffing and bed management (though some of these can be covered to a limited degree using basic DHIS2 forms). DHIS2’s role as a pragmatic, lightweight EMR can help to overcome traditional barriers to digitizing patient data at the primary healthcare service delivery level, while also enabling interoperability and integration with more comprehensive EMR software established at hospitals and other secondary/tertiary care levels.
The DHIS2 platform includes built-in functionalities that fulfill key requirements of facility-level EMRs, EHRs, and digital registries:





DHIS2 is designed with interoperability in mind, supporting data exchange through various formats via the open DHIS2 API–including support for common data standards such as FHIR–to facilitate a cohesive health information ecosystem. It integrates seamlessly with several established open-source EMR platforms (such as OpenMRS, OpenEMR, and Bamhni) and complementary national systems such as Civil Registry and Vital Statistics (CRVS) systems, lab information systems and master patient indices. It can be extended to connect with external digital tools that support functionalities like biometrics and advanced diagnostics. This helps countries reduce fragmentation and supports the creation of unified information architectures for patient data.
Here are some examples from a selection of countries that show how using DHIS2 for electronic patient records can make an impact on program efficiency, effectiveness, and cost.
You can also read additional articles and published research about the role and effectiveness of DHIS2 for patient-level data management:
Watch these informative webinars and presentations for useful guidance, lessons learned, and best practices.
A webinar by the Global Financing Facility that explores the different types of Health Information Systems (HIS) and explains how each type of system addresses different data use needs.
This session from the 2024 DHIS2 Annual Conference includes a discussion on how DHIS2 supports EMR use cases and real-world examples from Iraq, Somalia, the Maldives, and Palestine.
From the 2022 DHIS2 Annual Conference, this session explores the use of DHIS2 Tracker programs at the point of care in locations which have never had a digitized tool before.
Get started with DHIS2 for electronic patient records with these helpful resources:
The Tracker Implementation Guide contains useful information about planning and implementing DHIS2 systems for patient-level data.
Find useful resources and downloadable metadata to help you configure DHIS2 for patient-level data in key health programmes.
A tool for assessing a country’s readiness for implementing DHIS2 systems at different scales and levels of complexity.
The DHIS2 functionalities and features that support patient-level data management have been developed in response to the needs of countries in the Global South, and in direct collaboration with local stakeholders, as part of HISP UiO’s mission of supporting information system strengthening in LMICs.