Mali’s COVID-19 Vaccination Management System Highlights Importance of Local Ownership of DHIS2
Mali’s COVID-19 vaccination campaign shows how the combination of local capacity and DHIS2’s flexibility help countries adapt their health information systems to meet new challenges
At the end of February 2020, the first case of COVID-19 was recorded in West Africa. Mali detected its first case in Bamako on March 25, 2020. Access to vaccines is the key issue in controlling the pandemic. Mali was the first country in the Sahel to acquire COVID-19 vaccines with the delivery in March 2021 of 396,000 doses of AstraZeneca vaccine from the COVAX initiative, launching a large-scale vaccination campaign.
Choosing DHIS2 based on local needs, local capacities and local ownership
In Mali, a scientific committee made up of executives from the Ministry of Health, academics and partners was created at the start of the pandemic to coordinate activities related to the management of the COVID-19, including establishment of health protocols, communication planning and response, data collection and management of immunization.
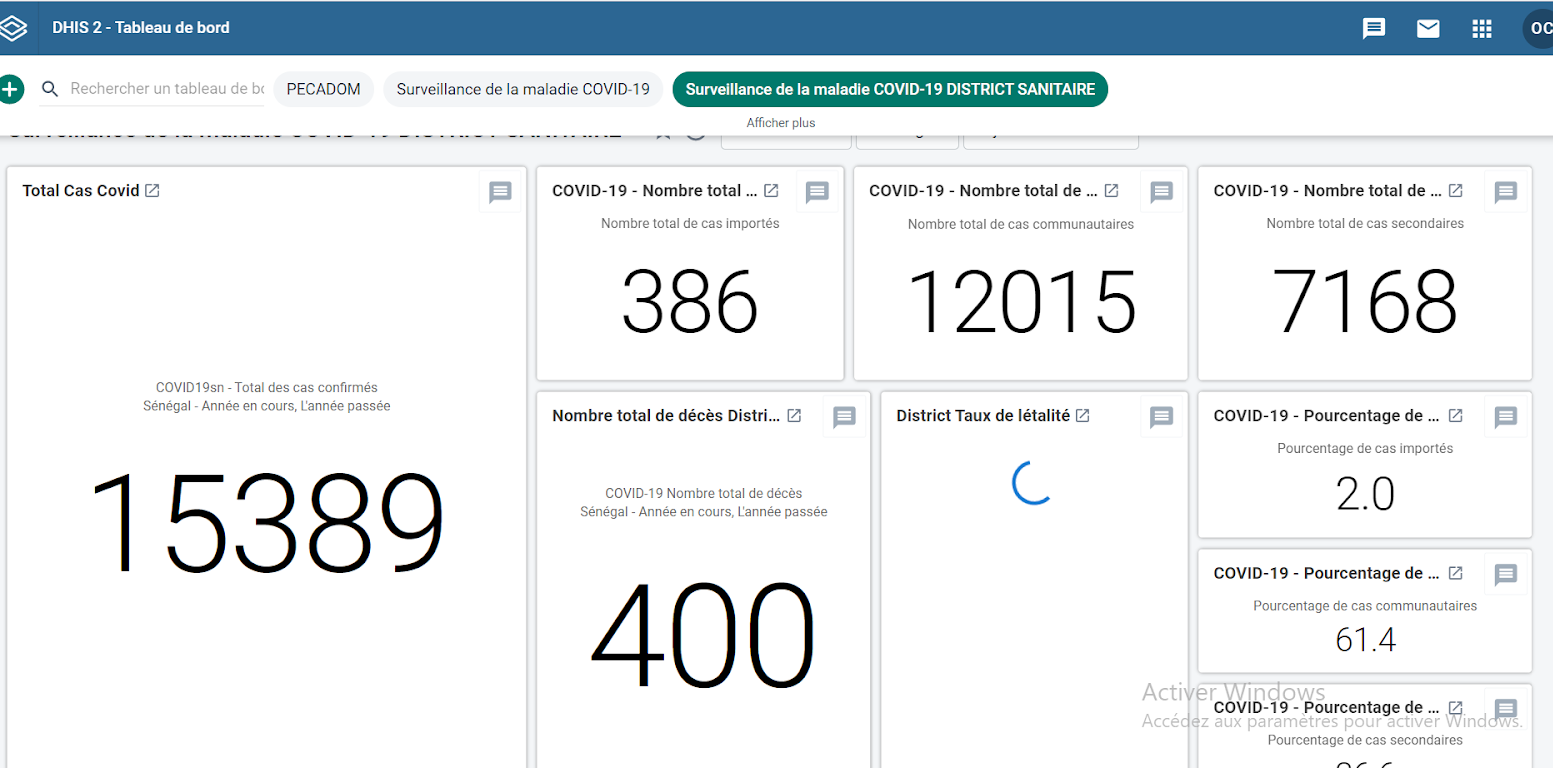
DHIS2 was identified by the committee as an obvious choice for the country’s vaccination strategy in order to reach 100% national coverage, due to the simplified access to data and storage of historical data offered by DHIS2, as well as data confidentiality features. The flexibility of the the DHIS2 software allowed it to be adapted to the needs of the country and deployed at the national scale. The data entered into DHIS2 is tracked and analyzed through DHIS2’s built-in analytics features, facilitating decision-making at upper levels.
The DHIS2 system deployed at the start of the COVID-19 pandemic was based on the WHO standard surveillance package and adjusted to the local context. With the support of HISP WCA, package deployment was initiated through the following actions:
- Configuration and validation of data entry forms with the import of the DHIS2 COVAC package onto the Mali server and the testing by the country’s Technical Team.
- Configuration of aggregate forms: population, daily vaccine distribution report and stock management.
- The configuration of Tracker for the design of the electronic vaccination registry as well as notification and investigation of AEFI cases.
In addition, Mali decided to establish an electronic health pass based on data from DHIS2. Data entry workshops have been planned with the aim of integrating aggregated historical data and Tracker data into the database, thus allowing the generation of health passes.
The health pass is being planned at the level of the Ministry of Health and Social Development. It will include information on the series of vaccinations and COVID tests carried out, and includes a secure QR code for reading and certifying information at airports and other dedicated control points. There is no regional standardization yet. Mali is planning to implement a health pass that meets EU standards, as one of the first West African countries to do so.
Launch of the COVID-19 vaccination campaign with DHIS2

The country launched its first COVID-19 vaccination campaign on March 31, 2021, with a first phase that was planned to last around 100 days. Faced with a limited vaccine stock at the start of the campaign, the political and health authorities decided to make the vaccine available to priority target groups such as health personnel, people over 60 years of age and those with comorbidities. The package has been configured to include these categories in dashboards to display the vaccination status of each group in real time. 173,242 people received their first dose during this campaign.

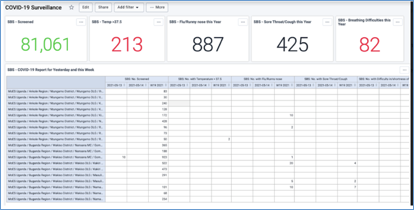
When a patient receives a vaccine in one of the health facilities or in one of the mobile centers, the information is entered first on the primary collection media (such as the vaccination register or vaccination record), then entered into DHIS2 by the health worker. This includes the patient’s personal information, the type of vaccine administered, the date of vaccination as well as the date of the second appointment. The patient’s immunization status and appointment details are linked to their individual record in Tracker. Aggregate data (such as number of vaccinated disaggregated by sex, age group and type of vaccine) is then collected and entered by the Technical Directors of the health centers and the HIS managers of the health districts. DHIS2 is also used to track new infections, trace contacts, and monitor patients’ COVID-19 treatment.
Using the DHIS2 Android Capture App for better data entry
Shortly after the start of the campaign, unstable internet connectivity in several regions became a major challenge. This impacted real-time data entry, leading to issues with reporting timeliness in certain areas. To address this, Mali deployed the DHIS2 Android Capture App. This brought real added value, offering the possibility of entering data on mobile devices for all DHIS2 data models, including aggregate data and individual data for Tracker and Event programs. The app works in both online and offline mode, which means data and metadata are automatically synced as soon as internet access is available.
In April 2020, WHO provided around 200 tablets for health workers in the Bamako district as part of the data management for surveillance of COVID-19 cases. In December 2020, the Global Fund financed more than 600 tablets intended for Community Health Centers and Reference Health Centers as well as hospitals in 6 regions. However, as of October 2021, these tablets had not yet been delivered to the site or configured due to lack of funding. This hampered the implementation and progress of data management of the vaccination campaign. The configuration is planned for the end of 2021.
New priority target group
Before the launch of the second campaign, Malian health authorities broadened the priority targets to people aged 18 and over, including all professions. From the systems perspective, this change had a noticeable impact on data entry and configuration, including the adjustment of age groups as well as the update in the DHIS2 database for a harmonization between paper and electronic registers, requiring regular sessions to adapt and harmonize data collection forms.

On 5 August 2021, Mali received 151,200 doses of the Janssen COVID-19 vaccine, followed a few weeks later by 835,200 doses of SINOVAC vaccine and 79,200 doses of AstraZeneca vaccine, all through the COVAX initiative. These vaccines were planned for delivery during a new campaign extending over the entire national territory.
System implementation challenges in Mali
Political instability: Many changes in government have impacted long-term strategic vision and funding. Increased insecurity limits the population in its movements, preventing people from accessing vaccines. In addition, healthcare professionals cannot always travel to administer vaccines to support mobile vaccination strategies. This is a big challenge.
Need for continuous training: Staff within health facilities tend to change frequently. Regional and district health information system managers provide local training for new users.
Infodemic and disinformation on COVID-19: False information around COVID-19 and / or vaccines such as AstraZeneca circulated in large numbers on social networks and impacted the number of people receiving the second vaccine dose. Mali therefore experienced difficulties in utilizing all of the first vaccine doses before expiry. Mass communication (radio, television, community leaders) has been deployed, and the health pass coming into effect soon will be compulsory for travel.
Next steps
- Entering historical data: The vaccination register is the primary medium for collecting vaccination data. This information will be entered in Tracker for the follow-up of vaccinated persons and the generation of the health pass.
- Capacity building: 1,800 professionals from SIS, EPI managers and technical directors of centers in 10 health regions will be trained by central level administrators and the HISP team on using the electronic forms for COVID-19 surveillance cases and vaccination.
In 2016, Mali began using DHIS2 at a national level. With 100% deployment (hospitals, regions, health districts, health facilities, and private structures), DHIS2 integrates all the subsystems of the health information system (HIS) for data management of all diseases.
Benefiting from and contributing to a global public good
Mali was one of the first countries in the Sahel to deploy DHIS2 for COVID-19 surveillance and response in 2020. The country is supported by several partners who collaborate on health information system strengthening, including WHO, USAID, the Global Fund, UNICEF, GAVI, the World Bank and HISP WCA, which has helped improved the performance of the national health information system, providing quality information for decision-making and facilitating innovative management of health data in Mali. All these forces joined together to support the implementation of the COVAC package for the collection and analysis of vaccine data using DHIS2.
The Digital Public Goods Alliance (DPGA) is an international organization that promotes the use of digital public goods to create a more equitable world. In April 2021, the DPGA released a statement advocating the use of open-source tools for the delivery of COVID-19 vaccines, in order to strengthen digital cooperation and promote equitable distribution of vaccines around the world. Mali’s experience in using DHIS2 highlights some of the strengths of digital public goods. It is a perfect example of how open source digital public goods facilitate the sharing of knowledge, best practices and innovations.
Do you have questions or comments about Mali’s use of DHIS2 for the management of COVID-19 vaccination? Ask questions and join the discussion on the Community of Practice.