HISP Uganda: 10+ years of implementing sustainable information systems
In this interview, Dr. Prosper Behumbiize of HISP Uganda shares some of the highlights, learnings, and impact from more than 14 years of working with DHIS2. Their biggest success is facilitating locally owned, sustainable information systems.
This interview is part of a series of articles on HISP history and impact, published as part of a yearlong celebration of the 30th anniversary of HISP
What is the history of DHIS2 and HISP in Uganda?
Prosper: I started working with DHIS2 in 2009 while I was working with the CDC Uganda as the Health Informatics Team Lead; a position that required supporting the digitalization of the Health Management Information System (HMIS) for the Ministry of Health (MoH) Uganda. At that time, CDC Uganda was supporting the Ministry’s HMIS, which had been developed in EpiInfo, an access-based system for health data. We faced a lot of challenges capturing health facility data and aggregating it at the national level. This was because paper health facility reports would be sent to the district for aggregating, and subsequently, the aggregated district reports were sent to the national level, where they were finally captured in the EpiInfo system. With this approach, tracking timeliness and completeness, correcting missing data or identifying errors presented major data quality issues. Attempts to correct these issues required recompiling the entire district report. We could not afford to capture facility-level data in this system.
While pursuing my Masters Degree at the University of Western Cape in South Africa (Masters in Public Health) in 2009, I got introduced to DHIS v1 in a course unit led by some of the original DHIS champions (Calle Hedberg and Norah Stoops of HISP South Africa). DHIS2 was not fully developed and widely known at the time, so I organized a Skype call with Ola Hodne Titlestad and Dr. Knut Staring (of the University of Oslo), who shared with me and my CDC Uganda informatics team what DHIS2 was able to do, including additional functionalities beyond DHIS v1.4. In 2010, we prioritized the U.S. Government (USG) SI MoH support to focus on implementing DHIS2 in Uganda.
We began with resource mobilization, like the establishment of technical teams, spearheaded by CDC Uganda, to study DHIS2 functionality and align it to Uganda HMIS reporting needs, including logistics management for HIV commodities. The requirements were defined and compared to the existing system features. It was observed that DHIS2 would meet 80% of the reporting needs for all stakeholders, and thus DHIS2 was identified as the tool for HMIS data collection. Approval of this implementation was made by the Resource Center Assistant Commissioner (Dr. Eddward Mukooyo), and a core team – including MoH staff and partners – was trained by University of Dar es Salaam DHIS2 experts (Dr. Masoud Mahundi and Yusuph Kassim). We were able to customize the aggregate HMIS reporting tools, import legacy data, and roll out the system to all 120 districts in Uganda in record time – just 6 months – while in parallel, Lars Helge Øverland (the Lead DHIS2 Developer) supported the customization of the ARVs logistics ordering and reporting module (aggregate version). The scale-up was heavily facilitated by the USG Uganda implementation partners, who made sure their respective supported districts were equipped with internet and training in DHIS2 in addition to the equipment and support provided by the Government of Uganda.
With the inspiration of the then established HISP groups like HISP South Africa, HISP India and others, co-founder Dr. Fulgentius Baryarama and I started the process of setting up HISP Uganda, and officially registered the group in 2013.
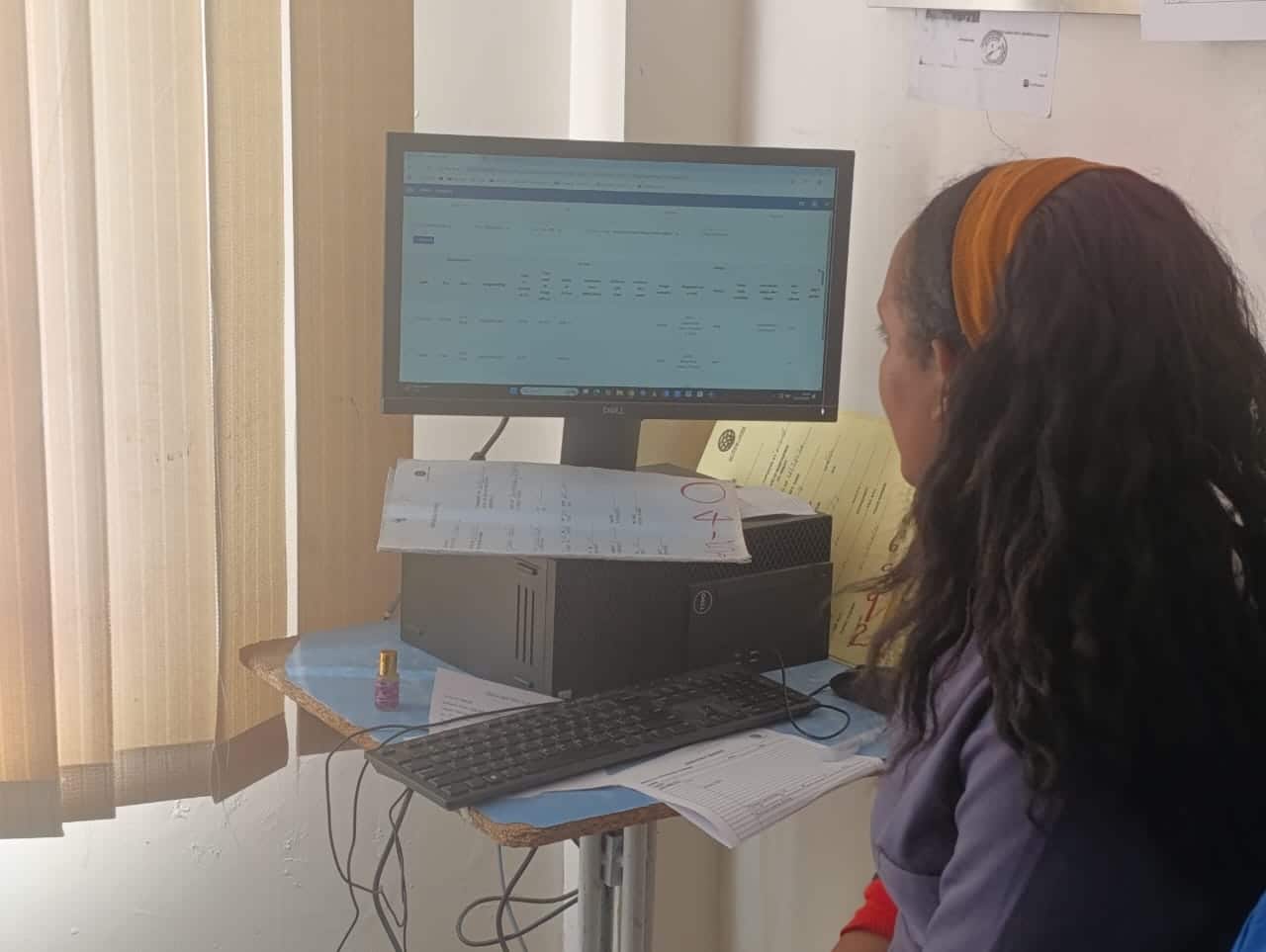
HISP Uganda has supported the MoH all the way from server management, DHIS2 configurations, resource mobilization, capacity building, analytics support, building dashboards, and more. We have trained over 1,500 Ugandans in DHIS2 through DHIS2 Regional Academies and national and sub-national trainings, primarily on topics including DHIS2 configuration, data capture, data analytics and more. We also provide help desk support to district users by phone, chat and email, which they really appreciate. A lot of our work has been pro bono to the government… but we do whatever we can to ensure that the MoH and now other Ministries (Education, Office of the Prime Minister, Office of the President) are supported when it comes to DHIS2 implementation.
Last year, in 2023, we celebrated our 10-year anniversary as a HISP group and received a lot of congratulations and recognition from the MoH, MoES, universities, US and UN agencies, and many partners about the added value they have seen in working with us.
“A big congratulations to HISP. I am very happy to be associated with your organization of a committed and focused team. You have enabled the MoH to pass through thick and thin paths on strengthening our HIS. We are proud of you and hope the collaboration grows stronger and stronger as there is still a lot we have to learn and innovate.”
Dr. Sarah Byakika – Commissioner of Planning, MoH Uganda

What is one project that has been a highlight of HISP Uganda’s work?
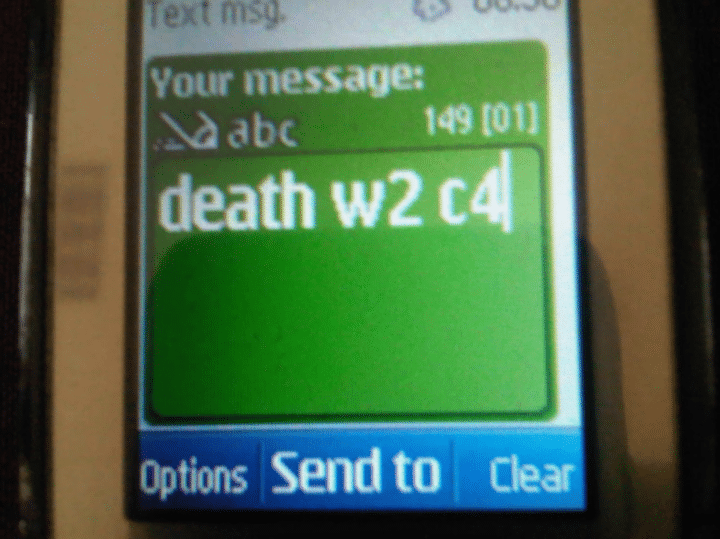
One of the projects that really highlighted HISP Uganda’s work was the Saving Mothers and Giving Life (SMGL) project. We got seed funding for this from Norad to support real-time, low-end SMS-based maternal and neonatal death reporting in the 4 project districts (Kyenjojo, Kamwenge, Kabarole, and Kibaale). We collaborated on this with a Masters student at UiO (Magnus Korvald) to finalize the development of the DHIS2 SMS functionality that was tested and fully implemented as a DHIS2 core feature. The project was able to achieve its objective of real-time reporting and conducting maternal and perinatal death reviews, aided by real-time data collection by community health workers. Ultimately, we were able to implement a module for sending data to DHIS2 by SMS that was used for daily reporting of any maternal and neonatal deaths from each of the four districts, and which was later scaled up to the entire country.
This ended up being a flagship project for HISP Uganda. The major outcome of this intervention was the adoption of SMS reporting into DHIS2 more broadly. This feature was later utilized in Uganda by the Emergency Operations Center for alerts on any events of public importance and the prevention of mother-to-child HIV transmission (PMTCT) program, which includes reporting data on stock and new cases reported on a daily basis. These projects are all still running today.
The lessons learned from this project have also been used in event-based surveillance, where the MoH and EOC in Uganda are using SMS alerts in the national DHIS2 system to alert district health teams and national stakeholders of any potential outbreaks. This has also been adapted in Botswana in the PMTCT program there, so this one particular activity has really impacted the way DHIS2 has been utilized beyond Uganda, especially for hard-to-reach areas with limited internet and electricity, where basic phones are the most reliable way to collect data.
We have further used the functionality and capacity in Uganda during the COVID pandemic to support disease surveillance, school-based surveillance, point-of-entry reporting and vaccination. It has also been adopted by all HISP groups in the network for reporting on surveillance and emergencies.
How have you supported sustainable digitalization and information systems architecture, including with other tools beyond DHIS2?
Our major goal has been to sustain DHIS2 implementation, not necessarily as a tool that just captures and stores data but, most importantly, to support the analysis and use of data. We have supported DHIS2 platform implementation by utilizing the core functionality and apps, but also by adding plugins and apps to extend its use. A lot of these extensions have focused on integration: trying to get data into DHIS2, so that it can serve as an integrated platform for health information. This includes getting data from other systems, such as laboratory information systems, Community Health Information Systems, EMRs (Uganda EMR, based on OpenMRS and the Clinic Master system, which is mostly used by private clinics) and others. HISP Uganda developed the award-winning Import Wizard app that has been used to integrate data from the various systems and apps that are being used to collect health data. For example, we used this approach to import ODK data for the Measles and Rubella real-time immunization campaign data management in 2018. We have also used the Import Wizard App to integrate data from lab systems such as ALIS for disease surveillance. Recently, the app was upgraded to include GoData data exchange functionality, and it has been used beyond health data exchange, for education and National Development Planning III financial systems data.
The major challenge we have is keeping up with the latest data visualization products. Most of the best visualization tools are very costly, as they are usually proprietary software systems that require user licenses and subscription fees; the MoH and most governments cannot afford them. With DHIS2, we have been able to build our own in-house visual studio app that provides similar features to the more expensive products like Tableau and PowerBI. We also developed an app to support real-time data visualization on smart displays, which has been used for immunization campaigns and outbreak management. Both this Smart Display app and the Import Wizard app are available on the DHIS2 App Hub for any country to download and use for free.
We have seen positive changes in data use thanks to these data visualization tools. For example, the EPI program strengthened their subnational data use through the Visual Studio app, which makes the data available in an interactive format at the district level. We recently completed an assessment of subnational data quality reviews, and we see the products we have designed being actively used. We have also seen improvements in data quality, for example, with more outliers and data errors being identified, and more frequent data calls that target some of the areas identified by DHIS2 visualizations.
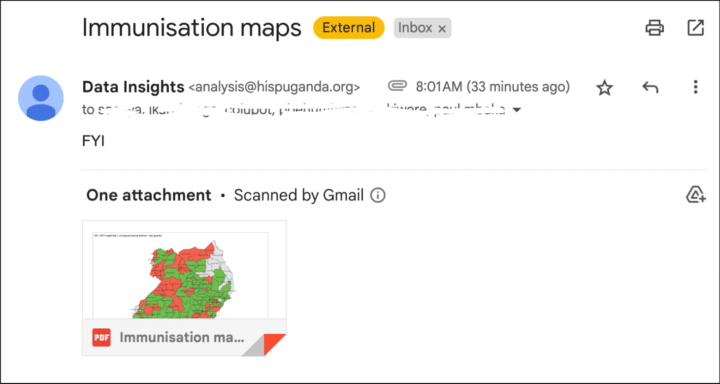
Access to data has also been a challenge for data use. Not everybody is able to access DHIS2 directly. So, we have worked on push analytics to automatically send visualizations from DHIS2 to stakeholders by email as pdf attachments. This makes it easier for them to access their dashboards from their email inbox without having to login to DHIS2. This is being piloted now.
How do you engage with the DHIS2 core team, the HISP network, and the larger DHIS2 community?
As HISP Uganda, we actively participate in the HISP network. This includes engaging in requirements gathering, testing DHIS2, and providing feedback to the software team through various structures and channels.
We’ve had quite a lot of interactions with the other HISP groups in the network through our Academy programs, where we come together and deliver global and regional academies. We communicate regularly and directly with the other HISP groups through WhatsApp and Slack. HISP Uganda, a regional HISP hub, has become a center of coordination for HISP groups in southern and eastern Africa. We have hosted meetings where the technical teams from different groups have come together, exchange visits, training sessions, and steering committee meetings — all of these help build capacity and share knowledge between the HISP groups.
We had also actively participated in the DHIS2 Community of Practice by sharing our innovations, use cases and implementations. Recently, we have focused especially on sharing updates on implementations beyond health that we are working on, such as education and government performance monitoring. This has led to individuals reaching out to us for demos or requests to help plan implementations or demonstrate them to other HISP groups and governments. These posts have also been a resource we can refer people to for information.
We have also presented at all the past DHIS2 Annual Conferences, including posters and oral presentation sessions, and at several DHIS2 Academies. Finally, we join the other groups during the HISP weeks and other strategic meetings organized by the HISP Center at UiO.
One of the strengths within the network is that we have been able to rationalize the HIS country support for different countries and domains amongst the HISP groups. We know who the experts are in different HISP groups, and we can look to them to help strengthen our capacity for working on specific technologies or use cases, just as other HISP groups can look to us for help. A recent example is a DHIS2 for Education grant we recently won in Nigeria as part of a consortium with HISP Nigeria and the HISP Centre. This is thanks to our combined experience and complementary skills and expertise. This is a good example of the strength of our collaborative network.

How would you describe your HISP group’s success or impact?
A key indicator of our success is that the information systems that HISP Uganda has helped implement have been sustained by the government and the different partners that own and use them. For MoH Uganda, which has used DHIS2 since 2011 as their main HMIS, we have focused on targeted capacity building to enable the maintenance of the system locally. The routine HMIS system management and maintenance are handled by the MoH teams. On occasions when we work on the system, such as version upgrades or other large updates, we work with Ministry staff in order to simultaneously train them so that they can do further customization and user support independently.
For our other partners, we have configured many DHIS2 instances and tools that have been used throughout their entire project cycles. For many of these, the systems are the sole source of data for the partners, and in some cases, they have been used for monitoring and reporting for more than 6 years. This has been attributed to the fact that one of the core attributes we include in our activities is capacity building for each project.
The majority of the systems we have built have revolved around HIV monitoring and the management of patients. We have built M&E tools for partners to be able to receive reports from implementing sites and report to their funders. We have built case-based surveillance systems such as TB that are still used and scaled nationally. We have always aimed to build capacity in the programmes and project teams to adjust the tools themselves, and this means that they have generally been able to sustain and support the systems on their own. Facilitating this kind of real local ownership of digital systems is one of our biggest successes.
Finally, having just celebrated our own 10-year anniversary, I think it’s important to recognize how we have succeeded as a team. HISP Uganda has attracted experts in the areas of software development, information systems analysis, implementation and support. We have been able to build a core of experts that has grown and become better and better at strengthening health information systems. Our team has been built to deliver quality work. In Uganda, this has earned us quite a lot of projects over time, especially with the government, to the extent that we now have MoUs with the MoH, Ministry of Education, the Office of the Prime Minister, and the key colleges of Makerere University: ICT and the School of Public Health. We have gotten contracts with WHO Uganda and Unicef — thanks in part to our MoU with the HISP Centre — and have also been able to acquire a number of projects and implementations as a sole source due to our positioning as DHIS2 experts in the region. To get this trust, you need to have a good team with quality outputs.

Do you have any closing thoughts to share with us?
As we move into the next decade as HISP Uganda, we really want to appreciate the HISP Centre at UiO for the support, capacity building and funding that have enabled HISP Uganda to deliver on a large number of assignments. We also want to appreciate the HISP Center for the mobilization of different partners who have invested in DHIS2, which has been a key digital platform to support developing countries. And we highly appreciate the DHIS2 community. It’s something that a number of other platforms have referred to as a good example of a community of practice that is constantly contributing to knowledge sharing. We have benefited from the community in terms of learning, sharing, and getting feedback that has improved our work.
Learn more about how the HISP Centre and the HISP groups collaborate to support countries worldwide on the HISP network webpage.